19-12-20:
Qualche altro ragguaglio arriva dalle lande svedesi, come se non bastasse quello che ho già scoperto al riguardo.
Ma tant'é, sappiate che c'é gente che NON ne vuole sapere di capire quanto gli svedesi siano nella cacca. Anzi, li difendono con argomenti ad minchiam, quando gli stessi svedesi NON hanno il coraggio di difendersi.
Perché lo sanno benissimo che hanno FALLITO miseramente.
E adesso vediamo perché.
Questa è la (invero succinta) relazione che la Commissione indipendente (il cui sito è questo: Coronakommissionen
Ha redatto sulla catastrofe sanitaria svedese. Quel che c'é scritto non è certo sorprendente, ma state sicuri, che per i 'credenti' della Svezia non basterà mai a dimostrare il contrario. I Guarini e guarinielli vari, insomma, dei fatti se ne fottono, se poi possono mettere in discussione le loro convinzioni.
IL PAZIENTE SVEDESE (ancora una volta)
Covid-19. Il caso svedese - SaluteInternazionale
- 30 Novembre 2020
La Svezia di fronte al fallimento della sua strategia basata sul no al lockdown. L’inutile sacrificio di migliaia di anziani.
La strategia anti Covid-19 della Svezia è stata fin dall’inizio la più discussa e controversa: senza lockdown, con bar, ristoranti, negozi vari e spazi pubblici rimasti aperti, con l’implicito obiettivo di raggiungere l’immunità di gregge, per garantire ai cittadini il massimo possibile di libertà e per salvaguardare – con le parole del governo – “jobs, businesses and economy”. Le domande sono: tali obiettivi stati raggiunti? e a quale prezzo?
In un video di 14 minuti Johan Carlson, direttore generale dell’Agenzia svedese di sanità pubblica, presenta le linee generali e le motivazioni della strategia, con le poche, specifiche disposizioni per il controllo della pandemia. Un video in lingua inglese, con sottotitoli in inglese.
Ricapitolando: la strategia anti Covid-19 del governo svedese, suggerita e sostenuta dell’epidemiologo Anders Tegnell, non prevede lockdown sul modello di vari paesi europei, ma solo alcune prescrizioni:
- Divieto di far visita nelle residenze per anziani
- Didattica a distanza per le scuole superiori e la parziale chiusura delle università
- Divieto di riunioni con più di 50 persone
- Le persone ultra70enni rimanere a casa e evitare i contatti sociali
- Rimanere a casa in presenza di sintomi lievi, e per due giorni dopo che uno si sente bene
- Mantenere il distanziamento fisico
- Lavarsi frequentemente le mani
- Evitare i viaggi non necessari
- Favorire il lavoro a distanza
“Alla base della strategia del governo svedese”, scrive Haba Habib in uno dei due ampi reportage del BMJ dedicati al caso svedese[1] “sta l’implicita e controversa idea che, piuttosto che contenere la diffusione di un’infezione, un paese può raggiungere l’immunità di gregge consentendo che una parte della popolazione s’infetti, a spese della morte dei più vulnerabili. Ciò non viene detto in maniera chiara e esplicita, ma l’immunità di gregge è l’obiettivo reale del governo svedese”.
L’immunità di gregge avviene quando una grande parte della popolazione (generalmente dal 50 al 90%, dipende dal tipo di infezione) si immunizza nei confronti di un’infezione e produce l’arresto della sua diffusione. Secondo i sostenitori di tale posizione questa strategia è più sostenibile nel lungo termine rispetto alle misure più dure adottate da altri paesi. E all’inizio sembrava funzionare, finché non si è assistito a un crescente numero di decessi: nella settimana tra il 25 maggio e 2 giugno la Svezia è stato il paese con il più alto numero di morti in Europa: una media di 5,29 morti al giorno per milione di abitanti (seguita dal Regno Unito con un tasso di 4,48). Come si può vedere chiaramente dalla Figura 1 il livello di mortalità della Svezia – dall’inizio della pandemia alla fine di novembre – è stato di gran lunga superiore rispetto a quello degli altri paesi scandinavi (tutti in lockdown) e della Germania, e non molto inferiore rispetto alla media degli altri paesi europei (Belgio a parte!). Va notato tuttavia che la Svezia al pari di Norvegia e Finlandia presenta livelli di densità di popolazione molto bassi (rispettivamente 23, 16 e 14 ab/km2), mentre quelli di Italia, Germania e UK sono 206, 232 e 278 ab/km2, e di Belgio è 345 ab/km2.
La mortalità tra gli anziani
In Svezia l’89% dei decessi si è verificato tra le persone con più di 69 anni, metà delle quali sono morte nelle residenze per anziani. Nonostante le prescrizioni/raccomandazioni del governo, il coronavirus ha liberamente circolato in questi ambienti per la mancanza di misure protettive, come le mascherine. Un operatore (anonimo) ha riferito al BMJ: “Il personale lavora fino a 14 ore con livelli di protezione sotto lo standard e continua a lavorare anche in presenza di sintomi”[1].
Ma gli anziani si sono ammalati e sono morti anche all’interno della comunità, soprattutto se esposte al contatto con persone più giovani, come figli e nipoti[2]. In Svezia si sono eseguiti pochi test, si sono considerati non contagiosi gli asintomatici e di conseguenza non sono stati messi in quarantena i “contatti” asintomatici (“The Public Health Agency of Sweden’s website states as long as siblings or other members of the family do not show symptoms of disease they can go to school, preschool, or their workplace.”, si legge nel citato articolo del BMJ), tutto ciò ha enormemente favorito la diffusione del coronavirus tra gli anziani.
Ma altri fattori sono entrati in gioco nell’eccesso di mortalità degli anziani, come la mancanza di terapie adeguate e di ossigeno all’interno delle residenze e l’atteggiamento “passivo” dei medici nei confronti dei pazienti anziani affetti da Covid-19. Yugue Gustafsson, professore di geriatria all’Università di Umea, notava che la percentuale di persone anziane in assistenza respiratoria a livello nazionale fosse più bassa rispetto all’anno precedente, nonostante le persone over 70 fossero le più colpite da Covid-19. Il professore esprimeva lo sconcerto nel constatare la crescente pratica dei medici di raccomandare al telefono la somministrazione di “cocktail palliativi” (a base di farmaci come morfina e midazolam, che inibiscono la respirazione) ai pazienti anziani[1].
Si sono raggiunti gli obiettivi?
Il sacrificio degli anziani e dei soggetti più vulnerabili è il prezzo da pagare nelle strategie che mirano a raggiungere l’immunità di gregge nel caso di infezione da Sars-Cov2. L’impegno del governo di tutelare questa fascia di popolazione non ha avuto successo. Un sacrificio inutile perché, nonostante le politiche di facilitazione della circolazione del virus, i dati ci dicono che i livelli di prevalenza dell’immunità da Sars-Cov2 sono lontanissimi dalle soglie dell’immunità di gregge: 7,1% a livello nazionale, 11,4% a Stoccolma e 6,3 a Göteborg[3].
Ma il sacrificio degli anziani, il prezzo da pagare per tenere aperta la società, non è servito neppure a tutelare il business e l’economia: nel secondo trimestre* del 2020 il PIL della Svezia è calato dell’8,6%, una riduzione peggiore rispetto a Finlandia e Norvegia (leggi qui e qui).
La seconda ondata
Alla fine di ottobre la seconda ondata è arrivata anche in Scandinavia. In Svezia, a causa dell’aumento dei casi, delle ospedalizzazioni e delle morti, nella maggioranza delle province, a partire dal 12 novembre, sono state adottate misure più restrittive: limitazioni nell’uso dei mezzi pubblici, no al contatto fisico con persone estranee al nucleo famigliare, massimo di otto persone ai tavoli di bar e ristoranti. La regione di Uppsala ha imposto restrizioni più dure e ha parlato di “local lockdown”, suscitando l’ira dell’Agenzia svedese di sanità pubblica che non vuole sentire neppure nominare il termine lockdown, e ha derubricato le misure come “stricter guidelines”[2].
I dati degli 14 ultimi giorni (fonte: Ecdc) parlano di 263 decessi in Svezia, contro 63 in Danimarca, 34 in Norvegia e 24 in Finlandia. Come scrive il Financial Times, il rapporto tra Governo svedese e Agenzia di sanità pubblica (che non accetta modifiche alla sua strategia) si sta incrinando. Ciò che preoccupa il Governo è il crollo di fiducia della popolazione sulla gestione della pandemia: ad aprile il 73% degli svedesi approvava le politiche del governo, a novembre il consenso è calato al 42%.
Summary SOU 2020:80 The elderly care in the pandemic (coronakommissionen.com)
Summary
Sweden is still in the midst of a major, widespread crisis. The coronavirus has made its way across the world, causing illness and death. The pandemic has also led to other far-reaching consequences for individuals and for the society at large, the scope of which we cannot yet fully comprehend. In parallel with the public debate on how this emergency is being handled, a number of countries have now embarked on a process of more long-term reflection and self-scrutiny.
At the beginning of December 2020, more than 7,000 people have died of COVID-19 in Sweden.1 Of these, almost 90 percent were aged 70 years or older.
Half of them were living in a long-term residential care facility (which encompasses nursing homes, care homes and sheltered housing), and just under 30 percent were receiving home help services. The large share of deaths among fragile elderly people is in line with observations from many other countries.
We find it most likely that the single most important factor behind the major outbreaks and the high number of deaths in residential care is the overall spread of the virus in the society.
The observation that the spread of infection in residential care follows similar patterns in several countries seems explicable.
The OECD states that the pandemic has highlighted a part of society that is undervalued and under-resourced.
The WHO also points to a number of common structural problems that have contributed to severe implication of the pandemic on people in residential care. However, not all countries have been equally hard hit, neither within nor outside of residential care.
There are also major regional differences within countries, and between different residential care homes. In this report we set out, in our view, the most important causes of the major spread of the virus and the high number 1 This includes all deaths where COVID-19 was reported on the death certificate, either as the underlying cause of death or as a contributing cause.
However, based on currently available evidence, we are not yet able to assess the relative importance of the different causes of the high numbers of cases and deaths in residential care and among those with home help services. Nor do we have data to evaluate some of the measures taken without a more comprehensive analysis of the spread of the virus in society in general, or an assessment of the more general handling of the pandemic.
We will therefore return to these questions in later reports.
The strategy of protecting the elderly has failed
The Commission’s overarching assessment can be simply summed up as follows: apart from the general spread of the virus in society, the factor that has had the greatest impact on the number of cases of illness and deaths from COVID-19 in Swedish residential care is structural shortcomings that have been well-known for a long time.
These shortcomings have led to residential care being unprepared and ill-equipped to handle a pandemic.
Staff employed in the elderly care sector were largely left by themselves to tackle the crisis. In Spring 2020, the Government and central government agencies put in place a number of measures to reduce the risk of spread of the virus in residential care (which in Sweden is carried out at the local government level). According to our overarching assessment, these measures were late, despite early information that older people were particularly vulnerable. We judge that the measures were also insufficient in several respects.
The view of the Commission is that the ambition of Sweden’s overarching strategy to specifically protect the elderly population was and is correct. Although Sweden, in comparison with other countries, does not stand out with a high share of deaths in residential care, it is nevertheless clear that, so far, this part of the strategy has failed.
Preparedness of the elderly care sector – structural shortcomings Fragmented organisation
In Sweden, crisis management is built on the principle of responsibility.
This means that the party responsible for a particular activity under normal circumstances, is also responsible for that activity in a crisis situation. This is a simple principle in theory, but the more people who share the responsibility, the harder it becomes to make the system as a whole work well in practice. In Sweden, responsibility for the health and care of the elderly population is decentralized to local government, which means that it is divided between 21 regions and 290 municipalities. Many regions and municipalities also have a large number of private providers. On top of this, there are the central government agencies with a national responsibility in these areas. When the spread of virus broke out, there was no overview at national level of the municipalities’ preparedness to tackle a pandemic.
The central government agencies concerned had not sought this information sufficiently early on, or to a sufficient extent, and if they had done so, it had not reached all the way to the parties involved. In the decentralized – and non-integrated – Swedish system the regional councils are tasked with the responsibility of health care, while the elderly care is mainly the task of the municipalities. However, it should be noted that the municipalities to a limited extent holds the responsibility for the health care in elderly care.
There was also a lack of established channels between, for example, the National Board of Health and Welfare and the municipal healthcare system similar to the channels in place between the Board and the regional healthcare system. When it comes to the division of responsibility between regions and municipalities, it has been asserted for many decades that these divisions lead to significant problems. In the past two decades, different studies and inquiries have shed light on the consequences that these shortcomings in coordination might have.
The regions’ responsibility for physicians and the municipalities’ responsibility for elderly care, illustrate the problems that arise when two principals simultaneously share responsibility.
The National Board of Health and Welfare and the Health and Social Care Inspectorate, have drawn attention to shortcomings in the lack of integrated care.
Even in normal times, the shared responsibility between different principals and a number of different actors presupposes good, trusting and continuous collaboration. In a pandemic – with demands for rapid prioritisation and knowledge transfer, and with a lack of necessary equipment – this division of responsibility makes even higher demands in terms of well-functioning organisations, coordination and collaboration.
A part of the Commission’s mandate for its future work is to evaluate how the crisis management principle of responsibility has worked during the crisis, and to propose measures that derive from these observations. In our view, as long as the current principle of responsibility applies, it is of utmost importance that coordination and collaboration between municipalities and regions work well, especially for tackling a crisis such as a pandemic.
There is a need for instruments and established institutional channels that ensure continuous operational coordination between regions and municipalities. All parties involved need to safeguard the whole system and invest in sufficient resources.
This is likely to require overarching changes in governance of elderly care, including medical care.
The lack of patient-centred, integrated patient medical records is a severe threat to the safety of patients.
The regions and the municipalities must take action to put in place systems for integrated medical records.
Need for higher staffing levels, greater expertise and reasonable working conditions
Major initiatives have been carried out during the pandemic to provide the elderly population with as good healthcare and social care as possible in the prevailing circumstances. Many employees have worked under extreme pressure, experienced fear and exposed themselves and their families to significant risk.
They have still done their utmost to meet the needs of recipients of healthcare and elderly care and to keep services running. Many managers and crisis management teams across Sweden have worked hard to find solutions in an unprecedentedly tough situation.
At the same time, the Commission notes that, in addition to nonintegrated responsibility for health and medical care, elderly care suffers from clear, major structural problems that the pandemic has.
The OECD and the WHO have described elderly care as an under-resourced part of society that is staffed by an undervalued team of professionals, and Sweden is no exception. The structural problems of elderly care that have been wellknown for a long time have to be addressed. It is necessary to increase the level of ambition and to raise the status of and the attractiveness of the caring professions to provide good quality healthcare and social care in a crisis such as the pandemic.
The Commission considers that the Swedish parliament and the Government must review what should be considered sufficient staffing rates in long-term residential care and in home help services, not least in terms of the care and treatment of people with dementia.
The employers must also better facilitate leadership by reviewing leadership structures and organisations such that managers are to be responsible for a much lower number of employees.
Furthermore, the employers must improve employment security and staff continuity in elderly care and sharply reduce the proportion of staff on zero-hours contracts. While it is hard to completely avoid using employees on zero-hours contracts who can be called in at short notice when required in as staff-intensive a sector as healthcare and elderly care, the proportion of staff on such contracts must be significantly reduced. Regarding the level of expertise in elderly care, the composition of workers from different professions clearly differs between the Nordic countries. Unfortunately, Sweden does not stand out in a positive sense in this respect.
Despite increased medical needs among recipients of elderly care in Sweden, the share of medically trained personnel is generally low. The view of the Commission is that medical expertise in elderly care needs to be increased.
This could be achieved, for example, by introducing a requirement on minimum training for different professional categories, and, in conjunction with this, considering the need for extra training initiatives. As a general rule, nursing skills should be available in all residential care facilities, round the clock, seven days a week.
Firstly, this is essential for access to medical interventions in the form of drips and oxygen, but also to ensure that other staff are able to obtain support and guidance in both care and in medical treatment. Furthermore, the municipalities must carry out language training initiatives for care staff who lack sufficient language skills. The vital increase in ambitions may demand the support of Government initiatives.
Inadequate regulatory framework
Many measures to prevent the spread of the virus in residential care for older people contradict the normative principles on which Swedish elder care is based. It is, at best, uncertain whether the legislation in place would allow for all the measures needed in these settings. Among other things, this involves arranging cohort care, i.e. where one or more people infected with the virus are cared for separately by staff who only work with these residents.
The view of the Commission is that, in an exceptional situation, a provider of health and elderly care must be able to take the restrictive measures required to effectively provide protection from the virus. However, it is evident that such restrictions on the freedom and rights of the individual must have legislative backing. It is not reasonable to delegate these difficult decisions to local politicians and employees. The current regulatory framework does not go far enough, nor is it clear enough. The legislator must therefore ensure that there are legal opportunities in elderly care to take the measures needed to protect recipients of social care in a pandemic and in other extraordinary crisis situations.
The possibility for municipalities to employ physicians and to access to medical equipment
The municipalities are one of the principals of healthcare for older people. The regions are however responsible for medical care provided by physicians. This responsibility may not be transferred to the municipalities. In principle, this presents an obstacle for municipalities in that they are unable to employ physicians for elderly care.
This makes elderly care dependent on the regions’ priorities for the kinds of medical assessments provided by physicians. It also means that in principle, physicians cannot be involved in the planning of healthcare within the municipality not even in the crisis management that the municipality has to perform during a pandemic.
No equivalent division in responsibility between different principals exists in our neighbouring countries.
The view of the Commission is that the categorical division between municipality and region in terms of responsibility for physicians does not appear to be an appropriate solution in a normal situation, and especially not in a crisis in which every step in the decisionmaking process and interface constitutes an inherent vulnerability. It is therefore the view of the Commission that it ought to be possible for municipalities to employ physicians.
The Commission further believes that all residential care for the older population should have the medical equipment necessary for medical interventions and good palliative care to take place on site. This includes apparatus for providing oxygen and nutrient solution. An apparent reason for this is that it would enable the resident to access such interventions without the potential stress of a hospital transport and a hospital stay.
Specific decisions and measures – late and sometimes insufficient
Attention was only paid to elderly care at a later stage Protecting the elderly population became an objective at an early stage of the pandemic. However, it took far too long before attention was paid to the specific problems and shortcomings in municipal elderly care.
The Commission can confirm that the main focus of the responsible government agencies in the early stages of the pandemic was on regional healthcare capacity. We believe that it was reasonable to prioritise the capacity of healthcare to treat serious cases of COVID-19 and to provide recommendations to the public aimed at limiting the spread of the virus. Still, it appears blameworthy that attention was not drawn to the conditions in residential care for consistently frail older people earlier, seeing as it was known that the consequences of infection were particularly severe in this group.
The Public Health Agency of Sweden and the National Board of Health and Welfare should have immediately placed more emphasis on conditions in Summary SOU 2020:80 8 residential care for older persons.
Our assessment is that these central government agencies did not have an adequate overview of the problems and deficiencies in municipal elderly care. This meant that guidance on measures in elderly care was delayed.
Problems with personal protective equipment
Access to personal protective equipment (PPE) was remarkably poor in the initial stage of the pandemic.
As early as February 4–6, both the Swedish Civil Contingencies Agency (MSB) and the National Board of Health and Welfare identified a risk that a deficiency in PPE could arise. However, it was not until early April, long after the virus had entered residential care for older people, that the National Board of Health and Welfare began to form an overview of the situation in the municipalities, via the county administrative boards which are regional government agencies. The view of the Commission is that it took an unreasonably long time to clarify and define the need for PPE in elderly care. Given the large number of municipalities and care providers in Sweden, channels for reporting such needs should already have been established or have been rapidly organised. However, these questions will be further examined in a later report. The same applies to issues regarding emergency stock, priorities in the event of a shortage and procurement or repurposing of production.
The question of which protective equipment was to be used when working with recipients of care who were suspected or confirmed to be infected with the virus was long disputed, and conflicts arose in several workplaces. The handling of the question of PPE in elderly care by the responsible agencies gave rise to a lack of clarity as to which PPE was appropriate. According to the Commission, it is reasonable to assume that the absence of clear guidelines and the obvious lack of PPE in elderly care contributed to the spread of the virus there.
There should have been early and consistent guidelines conveyed by both the Swedish Work Environment Authority and the Public Health Agency of Sweden surrounding the use of PPE. Alternatively, it should have been stated how the objectives of protecting staff and preventing the spread of the virus were to be weighed against each other.
The late introduction of testing In April, when the pandemic hit Sweden the hardest, no provision was in place for widespread testing. On March 30, the Government commissioned the Public Health Agency of Sweden to rapidly produce a national strategy for expanding testing. However, no such strategy was published until April 17. The reason for the delay and what was done on this issue before March 30 remains for the Commission to examine. We will also be investigating and evaluating several other aspects of testing and tracing and the question of whether the testing capacity that existed could have been better used had it been prioritised differently.
However, the Commission already considers that even with scarce capacity, all the older people who moved into residential care for the elderly and those who were discharged from hospitals and returned to their residential care home should have been tested without exception.
The ban on visits was imposed too late and was not re-evaluated often enough
The ban on visits to residential care introduced on April 1 was based on sound reasoning purely in terms of preventing the spread of the virus. It was known early on that COVID-19 posed a particularly serious risk to older people.
The Commission is not aware of any studies of the actual effects of the Swedish ban on visits to curb the spread of the virus to residential care facilities. International studies have not found evidence for such a ban being particularly effective. Even if the main routes by which the virus entered residential care have not been completely identified, it was reasonable to assume that relatives of the residents could bring the virus with them as it was prevalent in the general population. Therefore, it is the view of the Commission that imposing a national ban on visits was both understandable and defensible. If the ban is assumed to be effective, it also follows that a ban ought to have been imposed earlier, as did in fact happen in several municipalities and with several private principals. The Government should have allowed the decision to ban visits to apply for a considerably shorter time. A potential extension could then have been considered. The question of the existence of the ban and its limitations of individual rights could then have been more systematically assessed in relation to the general spread of the virus and the specific regional conditions.
The view of the Commission is further that in the government ordinance imposing the ban on visits, the Government should have made it clear that visits from relatives were to be permitted during the residents’ final days of life.
The fact that many people died without a relative by their side is unacceptable, even if the ban could be motivated as part of the strategy for limiting the spread of the virus. We intend to return to the question of whether there was legal support for the imposed ban on visits in a later report.
Other shortcomings identified
Guidelines regarding access to hospital care increase risk
Several regions issued guidelines or regulations on priorities. The governing regulations of Region Stockholm issued on March 20 have attracted the most attention. The regulations stated, among other things, that when deciding on hospital care, people in categories 1–4 on the Clinical Frailty Scale (CFS) were to be prioritised. Hardly anyone in residential care for the older people are in the prioritised categories. The Health and Social Care Inspectorate has shown that there was a marked reduction in the number of referrals to hospitals from residential care facilities for the older people during February–June 2020.
However, it is hard to establish whether this type of guidelines led to physicians failing to make individual assessments of care need – as dictated by guidelines issued by both the National Board of Health and Welfare and Region Stockholm. However, it is not possible to rule out the fact that such guidelines – combined with the lack of equipment and partly also staff needed for on-site medical treatment residential care facilities – may have contributed to decisions to administer palliative care instead of hospital care or other active disease-related treatment. The view of the Commission is that even in a pandemic, guidelines that risk using categories to determine the individual need for care should be avoided.
Even though the guidelines state that an individual assessment must always be made, there is a significant risk that this will not be done in a chaotic situation, in which there is a 11 demand for clear rules of action and a widespread concern that hospital beds and intensive care beds will run out, in combination with online assessments made without sufficient knowledge of the patient. The guidelines must always be drawn up with great care, emphasise individual assessment, avoid simple categorisations and be based on careful ethical considerations.
Lack of physicians present and no individual assessment by a physician
The investigation of patient records for 847 people in 98 residential care units by the Health and Social Care Inspectorate reveals up to about 20 percent of cases were not assessed by a physician at all. In 40 percent of these cases, there was no individual assessment by a nurse either. Furthermore, the investigation shows that not even 10 percent of the patients/recipients of care were assessed at the residential care facility. It is the view of the Commission that it is unacceptable that there have been cases in which the resident was not individually assessed by a physician and in some cases was not medically examined at all. Assessment by a physician online is particularly problematic concerning potential hospital admissions. It is likely that the risk of incorrect assessments being made on this issue has been greater during the pandemic, in part due to all the unknown factors surrounding the disease. According to the Commission, it is unacceptable that so many assessments were made online by physicians who lacked previous knowledge of the patient.
Responsibility for the shortcomings
We have found that elderly care was unprepared and ill-equipped when the pandemic struck and that this was founded in structural shortcomings that were known long before the outbreak of the virus.
The ultimate responsibility for these shortcomings rests with the Government in power – and with the previous governments that also possessed this information. The Government governs the Realm (Chapter 1, Section 6 of the Instrument of Government) and Summary should therefore have taken the necessary initiatives to ensure that elderly care was better equipped to deal with a crisis of this nature.
Non bastando nemmeno questo, ecco a voi cosa succede nel campo della sanità (e quindi: mò so cazzi...):
Sweden faces a 'terrible' reality as health-care workers quit - MarketWatch
Sweden faces a ‘terrible’ reality as health-care workers quit
Dec. 14, 2020 at 1:08 p.m. ET
By Shawn Langlois
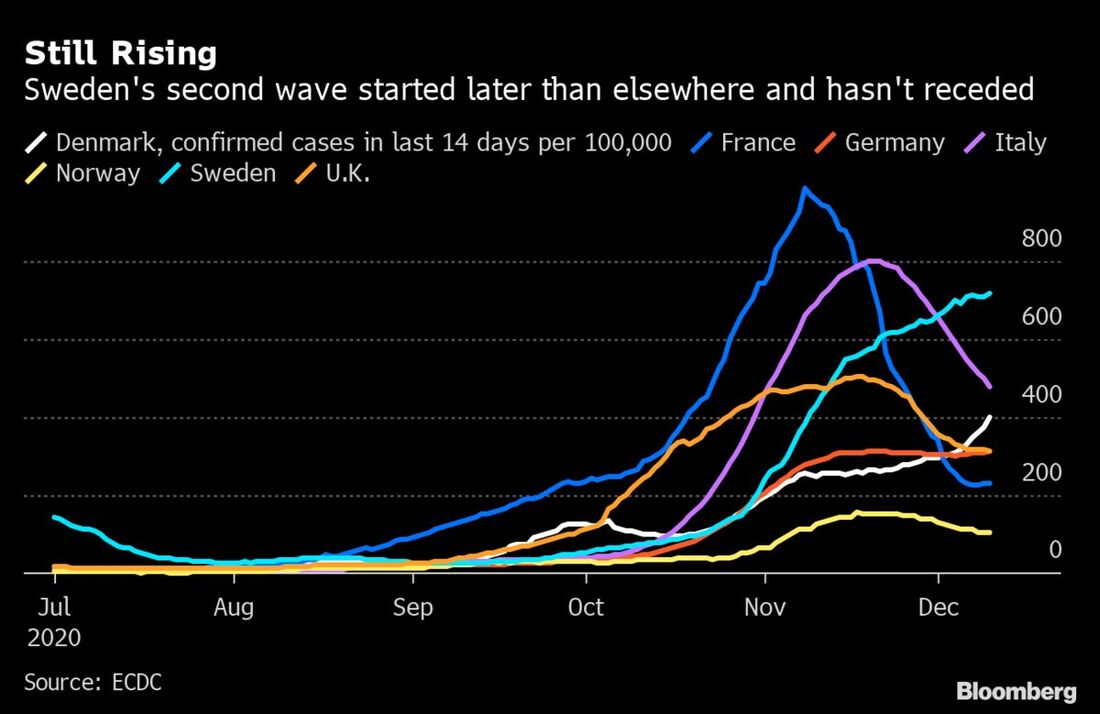
‘I talked to members in August who said they would resign because it was the only way to get some time off and recover. We see high rates of sickness, symptoms of exhaustion and members who have been infected.’That’s Sineva Ribeiro, the chairwoman of the Swedish Association of Health Professionals, talking to Bloomberg about the “terrible” situation in Sweden as coronavirus infections continue to spread.
She explained that there was “a shortage of specialist nurses, including at ICUs,” even before the pandemic hit back in March. With Stockholm’s intensive care capacity reaching 99% last week, the capital city is calling for outside help to handle the increasing number of patients.
As you can see from this chart, the trend is troubling:
Bloomberg highlighted a survey by broadcaster TV4 showing 13 of Sweden’s 21 regions saw a jump in resignations in the health-care profession from a year ago, at as many as 500 a month.
Also read: Bill Gates gives some ‘bad news’ on the pandemic
“In a work environment where you are so tired, the risk of mistakes increases,” Ribeiro said in the interview. “And those mistakes can lead to patients dying.”
Meanwhile, the U.S. still holds the highest case total in the world at 16.26 million, with almost 300,000 deaths, which is roughly a fifth of the global totals, according to data aggregated by Johns Hopkins University. There were a record 109,331 COVID-19 patients in U.S. hospitals on Sunday, topping the record of 108,487 set a day earlier.
The grim totals come as the first COVID-19 vaccine shipments began over the weekend.
Swedish Covid Workers Are Quitting, Leaving ICUs Short-Staffed (bloombergquint.com)
Sweden’s Covid Workers Are Quitting in Dangerous Numbers
Niclas Rolander Bookmark December 12 2020 --
Sweden faces a shortage of health-care workers as the number of resignations ticks up after a relentless year of caring for Covid patients. Sineva Ribeiro, the chairwoman of the Swedish Association of Health Professionals, says the situation is “terrible.” Even before the first wave of the pandemic back in March, there was “a shortage of specialist nurses, including at ICUs,” she said in a phone interview. The development shows that even countries with universal health-care systems are struggling to keep up with the Covid crisis. This week, Stockholm’s intensive care capacity hit 99%, sending the city into a panic and prompting calls for outside help. But even if more ICU beds are provided, the bigger concern now is whether Sweden has enough health-care workers with the skills needed to needed to look after the country’s sickest patients.
The worry is that, despite scientific strides that allow medics to better understand and treat Covid-19, there aren’t enough professionals left to put that knowledge into practice. “We don’t have the staff to do it,” Ribeiro said. She described the current health-care crisis facing the country as “unprecedented.”
Ribeiro says that already back in May, members of her union “warned of an untenable situation.” There are fewer qualified people available now than there were in the spring, “which makes it harder to expand ICU capacity,” she said.
Health-care professionals have emerged as the heroes of the Covid crisis, often drawing cheers from grateful onlookers as they emerge from hospitals after long and grueling shifts.
But increasingly, staff are so desperate for some real time off that they see resignation as the only way out, Ribeiro said. A survey by broadcaster TV4 showed that in 13 of Sweden’s 21 regions, resignations in the health-care profession are now up from a year ago, at as many as 500 a month.
The Army Stockholm County Mayor Irene Svenonius says the situation is “extremely tense.” In an interview with Dagens Nyheter on Friday, she acknowledged that health-care workers are overworked, and that there’s a need to add staff. “There’s fatigue,” she said. “You can’t ignore that, so it’s extremely important to get more people.”
It’s uncertain where that extra capacity will come from. Stockholm has asked for additional health-care staff from Sweden’s armed forces, but it’s not clear the military has the resources to help. In the meantime, over 100 staff from a children’s hospital have reportedly been redeployed to intensive care units, meaning that children who had been due to receive non-emergency surgery will now be forced to wait.
On Saturday, neighboring Finland said it’s ready to assist by freeing up space for Swedish ICU patients. But before Sweden draws on help from its Nordic neighbors, it will try to use available ICU capacity in parts of the country that are less burdened, according to local media.
The worry is that, despite scientific strides that allow medics to better understand and treat Covid-19, there aren’t enough professionals left to put that knowledge into practice. “We don’t have the staff to do it,” Ribeiro said. She described the current health-care crisis facing the country as “unprecedented.”
Nurse’s Pay
Part of the problem is that nurses in particular are increasingly unwilling to subject themselves to the hours and conditions facing them during the Covid crisis, given the average pay level. Sara Nordin, once an assistant nurse at an intensive care unit, told Bloomberg in October that she quit because she couldn’t make ends meet on the $33,600 basic pay she got a year. “I talked to members in August who said they would resign because it was the only way to get some time off and recover,” Ribeiro said. “We see high rates of sickness, symptoms of exhaustion and members who have been infected.” For Sweden, the danger now is that more people will die because there aren’t enough qualified health-care professionals left to look after them.
“In a work environment where you are so tired, the risk of mistakes increases,” Ribeiro said. “And those mistakes can lead to patients dying
Economia, almeno quella... macché:
Già a luglio:
Sweden's COVID-19 strategy left many dead, no economic gain: data - Business Insider
Sweden's controversial anti-lockdown strategy resulted in a high death toll and no real economic gain, data shows
Rosie Perper
Jul 9, 2020, 8:31 AM
- Sweden's unusual coronavirus strategy has not resulted in significant economic gains, data indicates, and has instead left the country with a far deadlier outbreak than its Nordic neighbors.
- Sweden has never issued a formal lockdown and has instead encouraged its citizens to stay home when they're sick and maintain social distancing when in public.
- But Sweden's coronavirus mortality rate is among the highest in the world, and, according to Reuters, Sweden's central bank this month forecast that the country's economy would shrink by 4.5% this year.
- Jacob Kirkegaard, a senior fellow at the Peterson Institute for International Economics in Washington, told The New York Times that Sweden "literally gained nothing" economically from the risky policy.
Sweden never issued a formal lockdown in response to the coronavirus pandemic. Instead, the country's coronavirus model has relied on personal responsibility and encourages citizens to stay home when they're sick and maintain social distancing when in public. Most businesses, restaurants, bars, and schools have remained open, though gatherings of more than 50 people were banned in late March.
Swedish Prime Minister Stefan Lofven defended the policy as "common sense" that allowed the country to maintain the status quo.
But the unconventional strategy has faced some pushback from experts, who have said the policy, in hindsight, "maybe hasn't been the smartest in every respect."
Jacob Kirkegaard, a senior fellow at the Peterson Institute for International Economics in Washington, told The New York Times in an article this week that even though industries remained largely open and unchanged, Sweden did not see significant economic gains.
"They literally gained nothing," Kirkegaard said. "It's a self-inflicted wound, and they have no economic gains."
According to Reuters, Sweden's central bank this month forecast that the country's gross domestic product — a measure of the size of a country's economy — would shrink by 4.5% this year, contrasting with a previous prediction that its GDP would rise by 1.3%. The Times added that Sweden's unemployment rate rose from 7.1% in March to 9% in May.
As of June 8, Sweden had reported more than 73,000 coronavirus infections and more than 5,400 deaths, according to Johns Hopkins University — higher than all of the other Nordic countries combined.
Sweden's coronavirus mortality rate, which accounts for deaths as a share of an overall population, has also been among the highest in the world.
According to figures from Our World In Data, an online research publication based at the University of Oxford, Sweden has confirmed more deaths per million people than the US, Brazil, India, and Russia, all countries with significantly higher death tolls overall than Sweden.
Some Swedish officials have urged the country to reconsider its coronavirus strategy.
In April, more than 2,000 Swedish scientists signed open letters urging the country to reconsider a lockdown.
Sweden's former state epidemiologist Annika Linde told the local newspaper Dagens Nyheter in May that she believed the country "should have imposed significantly tougher restrictions from the beginning."
"We should have known how underprepared we were in healthcare, and elder care," Linde told the paper. "A shutdown could have given us a chance to prepare ourselves, think things through, and radically slow the spread of infection."
Sweden Covid-19 Resurgence Will Hurt Economy in Months Ahead - Bloomberg
Sweden Warns of Covid Hit to Economy After ‘Unprecedented’ Curbs
18 novembre 2020, 14:36
Sweden’s government has acknowledged that the latest Covid-19 flare-up means the economy will be weaker over the coming months than previously thought.
Finance Minister Magdalena Andersson said the pandemic is now “just as serious” in Sweden as it was back in March and April. “The transmission we have seen recently, and the measures taken here and in other countries, are expected to dampen the economic recovery,” she said at a press briefing on Wednesday.
Sweden has so far faced a milder recession than many other European nations, after leaving much of its economy open throughout the pandemic. But with new cases soaring and hospitals filling up as Europe enters winter, the outlook is now much bleaker.
On Wednesday, Sweden reported 96 deaths due to Covid-19, and fatalities are now at a level not seen in the country since June.
The number of Covid patients in Sweden’s intensive-care units has doubled over the past 13 days. The overall level remains well below a peak in April, but the development has triggered dire warnings from the government that Sweden is now facing a “really dark” winter.
Sweden has so far relied on mostly voluntary measures to encourage social distancing. But this week, it took the “unprecedented” step of banning public gatherings of more than eight people, in an effort to fight the virus. And Prime Minister Stefan Lofven has urged Swedes to “cancel” any social activity that might fan infection rates.
Read more: Sweden Uses ‘Unprecedented’ Covid Restrictions as Cases Soar
The stricter measures, while needed to fight the virus, are likely to dent economic growth, Andersson said. But she also noted that the rebound seen during the summer months was stronger than expected, meaning it’s not yet clear how much full-year forecasts will need to be adjusted. The Finance Ministry’s latest estimate for 2020 points to a 4.6% contraction.
Un ultimo appunto per la Svezia.
Spesso si sentono fare comparazioni tra Svezia e Italia, ovviamente loro hanno avuto 'meno morti di noi' e 'non hanno fatto il lockdown'.
Ma quando la premessa è sbagliata, anche la conclusione lo è.
E il lockdown o no, non è una premessa accettabile, quando per il resto si parla di due nazioni del tutto diverse per: latitudine, clima, genetica, cultura, geografia.
Facciamo qualche esempio pratico?
Se i fan(atici) della Svezia 'che non fa il loccdaun' sono così contenti di quel che hanno fatto loro, almeno stessero zitti su tutto il resto.
Ma no.
Se gli fai notare che ci sono nazioni che hanno fatto meglio di loro, rispondono invariabilmente che o hanno fatto il lockdown oppure sono MENO popolate della Svezia.
A parte che ho già detto quel che penso: devi essere proprio un gran figlio di un cane rabbioso, per essere favorevole alla morte di migliaia di persone 'vecchie', spesso addirittura 65enni non curati e non visitati e non trattati nemmeno con una bombola d'ossigeno... per fare il picnic di fine settimana, anzi, l'happy hour. Queste immagini di svedesi felici che viaggiano con i capelli biondi al vento dovrebbero essere comparate con quello che passano i loro vecchi negli ospizi, ma visto che in Svezia c'é uno dei livelli di solitudine per la gente anziana, più alti che esistano al mondo, evidentemente non gli frega molto di questo dettaglio.
Individualità, già. Come dire che se guidi un'auto devi avere il diritto di andare dove vuoi, come vuoi, alla velocità che vuoi.E senza cinture, magari. A cosa serve la libertà, senza partecipazione e senza coscienza?
I semafori, le cinture, i caschi... sono tutti limiti, no? Perché non protestare contro di essi, oltre che contro le mascherine?
Perché in fondo è la stessa cosa. Mancanza di educazione civica e menefreghismo individualista.
Ma adesso torniamo alle nostre beghe standard, quelle della statistica.
Dunque, c'é gente che ti dice che la Norvegia no perché ha fatto il loccdaun (ah sì? Bah). Ma l'Australia no, perché ci sta una persona ogni 1.000 km (magari). Insomma, l'unico paragone valido è quello con l'Italia. Che però è una bestialità per le ragioni di cui sopra.
Adesso vediamo come se la cavano un pò di nazioni note per lo scarso numero di infezioni, con la famosissima Svezia.
-Svezia: 25 ab/kmq --- 789 morti x mln
-Australia: 3 ab/kmq --- 35 morti x mln
-N.Zelanda: 18 ab/kma --- 5 morti x mln.
-Italia: 200 ab/kmq --- 1120 morti x mln.
Tradotto: l'Italia ha fatto il 40% peggio della Svezia con 8 volte la densità abitativa.
140% vs 800%
La Svezia ha fatto 22 volte peggio dell'Australia con 8 volte la densità abitativa.
2200% vs 800%
La Svezia ha anche fatto 145 volte peggio della Nuova Zelanda con il 140% di densità abitativa.
14500% vs 140%
Comodo tirare fuori la densità abitativa solo quando fa comodo, eh?
E adesso andiamo a vedere anche le proporzioni tra nazioni scandinave:
-Norvegia: 15 ab/kmq --- 74 morti x mln
-Finlandia: 18 ab/kmq --- 88 morti x mln
-Danimarca: 137 ab/kmq --- 176 morti x mln
-Svezia: 25 ab/kmq --- 789 morti x mln
Quindi:
Svezia vs Norvegia: (NB: densità vs mortalità covid, Svezia come metro di paragone)
160% vs 1050% (= Svezia con densità +60% su Norvegia, ma mortalità covid al 1.050% ovvero di 10,5 volte)
Svezia vs Danimarca:
548% vs +448%
Svezia vs Finlandia:
140% vs 900%
Ne consegue che anche considerando la proporzione della densità geografica, 2 delle tre nazioni limitrofe hanno fatto nettamente meglio della Svezia.
Il resto sono le chiacchiere dei fan svedesi. Sconfessati anche dal Re di Svezia.
**************************************************************************************************************************************************************************************
NEGLI USA E' UNA TORRE GEMELLA OGNI 14 ORE
MA PURTROPPO la Svezia non è l'unico caso 'speciale da seguire' nel mondo. Gli appestati N.1, almeno come numeri assoluti, sono sempre gli States.
E la situazione è catastrofica. Realmente. Quando senti dei 'numeri' non ti rendi conto.
Quando vedi CHI rappresentano quei numeri, beh... è ORRIBILE. Altro non dico.
The Thanksgiving coronavirus death surge is here, and it's horrific - Business Insider
The Thanksgiving surge in coronavirus deaths is here. It's 'horrifically awful,' a hospital chaplain said.
Morgan McFall-Johnsen
9 hours ago
- More than 47,000 people in the US have died from COVID-19 since Thanksgiving.
- The virus has become the country's leading cause of death.
- It's just the beginning of the effects of Thanksgiving travel and gatherings, one epidemiologist said. The rate of death probably won't slow anytime soon.
- At some hospitals, staff can't keep up, and they say patients are falling through the cracks.
- Visit Business Insider's homepage for more stories.
"She was totally cheerful," Stacey told Business Insider. "I was astonished at how happy she was in that place, and I was impressed with how well they did at keeping the pandemic out."
But a few weeks ago, everything changed.
The Monday after Thanksgiving, a social worker at the nursing home called Singer DeLoye in tears. The worker told her that Marilyn, at age 80, had tested positive for COVID-19.
"They thought Mom was going to rally, but she wasn't rallying," Singer DeLoye said. "She seemed to be very, very tired and she was declining."
On December 6, the nursing home called again: It was time to say goodbye. Marilyn was unconscious. Stacey's brother Scott grabbed an iPad, donned a mask, and went into their mom's room in the COVID-19 ward. He video-called Stacey and all of Marilyn's grandchildren.
"When she'd breathe in and breathe out, it sounded just like crackling cellophane," Stacey said. "We all told her we loved her. We all remembered a story about something she did that was really special to us."
An hour later, Marilyn died.
She's one of more than 47,000 people in the US who have died from COVID-19 since Thanksgiving.
On Wednesday, the US reported a record of 3,448 deaths. In total, more than 312,000 have died in the country since the beginning of the pandemic (though that's almost certainly an undercount).
This week alone, two school teachers in Texas who'd been married 30 years died together, holding hands. A convent in Wisconsin lost eight nuns. COVID-19 claimed a Chicago paramedic — the fire department's third coronavirus death. An elder of the Standing Rock Sioux tribe died of the virus, just a month after his wife.
This unprecedented and tragic surge in fatalities is, in part, a product of pandemic fatigue, cold weather that has led people indoors, and the patchwork nature state policies on masks and closures — many of which are quite lax. But these recent record-breaking days of death, in particular, are the result of infections contracted around Thanksgiving.
Despite CDC warnings to the contrary, an NPR analysis of mobile phone data found that 13% of Americans ventured more than 31 miles from home on Thanksgiving Day. That's not a huge drop from last year, when it was 17%.
But it's common knowledge that the most Thanksgiving travel comes in the days before and after the holiday. The Transportation Security Administration screened 9.5 million airline passengers during the 10-day Thanksgiving travel period. That's less than half of what the TSA reported in 2019, but it still included some of the busiest days since the pandemic began.
Cases generally take about two weeks to appear in official tallies, since the virus incubates in the body for an average of five days, then people usually wait a few days to get tested after symptoms appear. Then there's the multiday wait for results, and the subsequent process of reporting them to health agencies.
Deaths, in turn, generally follow one to three weeks after a rise in cases.
Like clockwork, that is what we're seeing now.
"Every floor I walked in today, everybody's completely full," Amy Carlozo, the chaplain at Swedish Covenant Hospital in Chicago, told Business Insider.
"This is so horrifically awful," she added.
Nursing homes and hospitals are overwhelmed
Singer DeLoye suspects that staffing issues over Thanksgiving week created an opening for the virus to get into her mom's facility. That week, Minnesota Public Radio reported that the state's nursing homes were experiencing severe staffing shortages. This forced officials to call in the National Guard and email thousands of state employees in search of temporary staff.
With new people coming into a facility and understaffed workers spread thin, it can be difficult to spot new cases before patients infect others.
Scott Singer told his sister that there were 16 other patients on their mom's COVID-19 floor — one of two such wards in the nursing home.
Marilyn Singer's end-of-life isolation did not match the way she'd lived. She'd moved from place to place for most of her years — California, Portugal, Belgium, Illinois, Wisconsin, Florida. She went to business school (the first woman in her program, she always said), appeared as an extra in a few movies, and worked as an accountant. She'd given Stacey and Scott many of her own original oil paintings, which decorate the walls of their homes. She had four grandchildren.
Zoom goodbyes like the one those grandchildren had with Marilyn have become a daily occurrence for Carlozo. Cook County, where Chicago is located, has the third-highest death toll in the US at more than 7,500, according to Johns Hopkins.
Due to a shortage of N95 masks, Carlozo doesn't go into COVID-19 patients' rooms unless absolutely necessary.
"It's almost like doing your job with your hands tied behind your back," she said.
Instead, she stands outside and calls into the video meetings with family members.
"I just want to do one more thing, and I wish I could do that one more thing for every patient I've dealt with," Carlozo said. "The volume is just so large at times I feel like I can't do enough."
She also frequently calls relatives after a patient has died, to listen to their grief and walk them through the process of finding a funeral home. Sometimes it's the first time Carlozo is meeting them.
"That's kind of how fast some of this is going. We haven't developed a relationship with them before their loved one has passed," she said.
Horror in the hospital
Experts are not surprised that exactly three weeks after Thanksgiving, the number of COVID-19 deaths each day has hit a new record. The virus became the leading cause of death in the US this month, according to an analysis published Thursday in the Journal of the American Medical Association.
"I don't think we've seen the full brunt of what happened during Thanksgiving yet. I think we're beginning to, but it's probably going to continue for some time," Amesh Adalja, an infectious-disease expert at the Johns Hopkins University Center for Health Security, told Business Insider.
That's because the chain of cases from the holiday are still spreading. Yet hospitalizations were already at all-time high of more than 114,000 as of Thursday. Nearly 22,000 of those people were in the ICU, and more than 7,800 were on ventilators, according to the COVID Tracking Project. In Southern California, intensive-care units have no beds left.
"There's been times when we've had multiple patients having cardiac arrest at the same time, and we've had to really triage to figure out which patient to resuscitate first," Dr. Hari Reddy, the intensivist medical director at St. Bernardine Medical Center in San Bernardino, told The Los Angeles Times. "If there's multiple emergencies, I try to gauge which patient I can make the most difference in."
More than 180 hospitals in California have applied for waivers to bypass mandatory staff-patient ratios, the LA Times reported.
"If you have a heart attack, if you get into a car accident, if you fall off a ladder or have a stroke, we may not have a bed for you," Dr. Brad Spellberg, chief medical officer at Los Angeles County-USC Medical Center, said in a briefing on Friday.
It could get much worse
The upcoming December holidays could spread the virus even more than Thanksgiving, according to Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases.
"This cannot be business as usual this Christmas because we're already in a very difficult situation, and we're going to make it worse, if we don't do something about it," he told The Washington Post.
The Institute for Health Metrics and Evaluation projects that COVID-19 could kill about 148,000 more people in the US by February 1.
"It's gotten to the point where it's just sort of numbers whizzing by and charts showing, you know, this horrible curve," Singer DeLoye said. "The human toll is missing."
Adalja said he doesn't expect this surge to let up before the holidays accelerate it.
"There's a lot of transmission going on, and there are just so many vulnerable people getting hit with infections, that I think it's just going to be a continual surge that we face until we get to a point where enough people are vaccinated," he said. The earliest that could be, he added, is January.
Carlozo said she had planned to take time off around Christmas but has now decided against it.
"I don't want to not be there for my nurses and my patients and my staff," she said.
She's trying not to think about the further death her hospital might see in the weeks ahead.
"I can't live in the would've, could've, should've," she said. "I just can't watch the news anymore. I can't hear it. I can't hear the deniers. I went through my period of anger back in, you know, October and November, and I'm done. I'm done. I just need to take care of what's in front of me."
COVID-19 is the leading cause of death in the US — again - Business Insider
COVID-19 is the leading cause of death in the US — again
Morgan McFall-Johnsen
Dec 17, 2020, 5:38 PM
Aracely Iraheta touches the casket of her husband, Jose Agustin Iraheta, who died of COVID-19, in Malden, Massachusetts, May 12, 2020.
Brian Snyder/Reuters
- The coronavirus has surged to become the leading cause of death in the US again for the first time since spring.
- The COVID-19 death rate in the US is equivalent to a new 9/11 every 1.2 days.
- To turn this around, President-elect Joe Biden will need a strategy to unite all 50 states in tackling the pandemic, according to public-health experts.
- Visit Business Insider's homepage for more stories.
Since November 1, the virus has killed more people in the US than heart disease, cancer, chronic lower-respiratory disease, transport accidents, or suicide, according to an analysis published Thursday in the Journal of the American Medical Association.
The US recorded a record of 3,400 deaths on Wednesday, according to the COVID Tracking Project.
"The fact that a condition that was unknown a year ago now ranks as the leading cause of death at the end of this year is just shocking," Howard Koh, a professor at Harvard's T. H. Chan School of Public Health, told Business Insider. "We need to do everything we can to have this illness revert back to the unfamiliar condition it once was."
Koh was not involved in the new analysis, but he co-authored an accompanying opinion piece.
COVID-19 probably won't be the overall leading cause of death for 2020. But it will be close. The researchers behind the new analysis compared COVID-19 mortality in the US from March to October with leading causes of death during the same months in 2018, when the most recent data is available. Only cancer and heart disease killed more people during that time. For people aged 85 and older, the coronavirus was the second leading cause of death, after heart disease.
"Many, if not most, COVID-19–related deaths could have been prevented," Koh and his co-authors wrote. "Critical public-health strategies must remain a major societal focus for the present and future."
A new 9/11 every day
Gabriel Cervera calls the family of a patient who died in a COVID-19 unit at United Memorial Medical Center in Houston, Texas, December 12, 2020.
Callaghan O'Hare/ReutersThe COVID-19 death rate in the US has been equivalent to a new 9/11 attack every 1.5 days, according to the new analysis, though in the last week it has grown to a 9/11 about every 1.2 days.
The comparison is "tragically appropriate," said Koh, who was the Massachusetts Commissioner of Public Health during the attacks in 2001. Like the 9/11 attacks, he said, the pandemic "seemed to come out of nowhere." It has also "completely upended all aspects of life in our society, and it's going to have prolonged aftereffects for many, many years to come," he added.
Put another way, the daily death toll is equivalent to 15 passenger planes, each carrying 150 people, crashing every day.
Bodies wrapped in plastic line the walls inside a refrigerated trailer used as a mobile morgue by the El Paso County Medical Examiner's office in El Paso, Texas, on November 13, 2020.
Justin Hamel/AFP via Getty ImagesBut the official numbers are likely an undercount. Koh and his colleagues write that calculations of excess deaths caused by the pandemic probably underestimate the toll by at least 20%.
Overall, the pandemic will likely prolong a trend of declining life expectancy in the US.
"Good health is so fragile and we cannot take it for granted," Koh said. "Public health protects our good health, 24/7. When prevention works, absolutely nothing happens. And all you have is the miracle of a perfectly normal, healthy day. And that's what everybody is craving right now."
But the upcoming holidays and associated travel and gatherings will likely spur further spread of the virus.
"We would need the public to follow recommendations from all public-health leaders, led by the CDC, about restricting or canceling travel plans. Those recommendations were pretty much ignored over Thanksgiving," Koh said. "We just cannot repeat that again."
Uniting 50 states with 50 different strategies
Though the US comprises just 4% of the world's population, it accounts for 19% of global COVID-19 deaths. It has reported more deaths than any other country.
Michael Neel, funeral director of All Veterans Funeral and Cremation, looks at the casket of George Trefren, a 90-year-old Korean War veteran who died of COVID-19 in a nursing home, in Denver, Colorado, April 23, 2020.
Rick Wilking/Reuters
It certainly didn't have to be this way. At the national level, a lack of clear public-health guidance and a president who spread misinformation and downplayed scientific expertise hampered efforts to build a united front against the virus.
"We've had 50 states following 50 different strategies throughout 2020," Koh said. "That unfortunately ended up negating the impact of the shutdown."
Koh and his co-authors recommended a path forward that includes better coordination between federal, state, and local leaders to increase testing capacity and contact tracing, along with focused outreach about vaccines to communities of color. They also suggested the government should send more resources to overwhelmed hospitals and healthcare workers, along with passing a stimulus package to aid schools, businesses, and people facing eviction.
"The new president has to articulate a national strategy as step one," Koh said. "We have not had that consistent communication throughout the first 11 months of this pandemic, unfortunately."
President-elect Joe Biden has said that once he takes office, he'll institute a 100-day mask mandate, distribute 100 million vaccine doses in 100 days, and make opening schools a priority. Biden has also pledged that his administration will enlist more contact tracers and establish emergency funding sources for vulnerable Americans and essential workers.
With the recent authorization of Pfizer's COVID-19 vaccine, a light flickers at the end of the tunnel. Moderna's is likely to follow suit this week. US officials estimate they will be able to vaccinate 20 million people — primarily frontline healthcare workers and nursing-home residents — by the end of December.
"I'm hopeful that 2021 will be a much better year and that next year will end with this pandemic largely behind us," Koh said. "But that will only happen if we rally as one nation and tackle this pandemic in a united fashion."
Notizie di cronaca (molto tristi):
8 nuns at Wisconsin convent die of Covid in past week, 4 on same day (nbcnews.com)
8 nuns at Wisconsin convent die of Covid in past week, 4 on same day
School Sisters of Notre Dame of Elm Grove said there were confirmed cases among the 88 sisters living at the facility, but did not specify the number.
00:26 /02:26
4 nuns from Wisconsin convent die of Covid on same day, 8 in a week
DEC. 18, 202002:26
By Wilson Wong
Eight nuns died from Covid-19 complications in the past week at a Wisconsin convent — four of whom died on the same day.
The convent, School Sisters of Notre Dame of Elm Grove, about 10 miles west of Milwaukee, said there were confirmed cases among the 88 sisters living at the facility, but did not specify the number, NBC affiliate TMJ4 reported.
Debra Sciano, provincial leader of the School Sisters of Notre Dame Central Pacific, told the station the eight sisters were all educators and “role models” who dedicated their lives to the community.
“For me, these are wisdom figures — women I have known for all of my 40 plus years in the community,” she said. “Every one of our sisters is really important, not only to us but feel they have touched a lot of lives we'll never be aware of.”
Eight sisters at Notre Dame of Elm Grove die from COVID-19 complications.WTMJ
The facility was first established as an orphanage, which later became a retirement home for elderly and ill sisters, according to the organization’s website.
Across the U.S., many nursing facilities for elderly people have been ravaged by the coronavirus.
The congregation said all the sisters followed public health guidelines outlined by the Centers for the Disease Control and Prevention, including wearing masks, social distancing, and regular handwashing.
Texas couple of 30 years die of Covid-19 within minutes of each other while holding hands (nbcnews.com)
Texas couple of 30 years die of Covid-19 within minutes of each other while holding hands
“It did give us some sense of closure that they both went together," one of their sons said.
Paul and Rosemary Blackwell
Dec. 17, 2020, 3:11 AM CET
By Stefan Sykes
A Texas couple married for 30 years who were hospitalized with Covid-19 were holding hands as they both died on Sunday, their family says.
Paul Blackwell, 61, and Rosemary Blackwell, 65 — longtime educators of Grand Prairie Independent School District — died just minutes apart at Harris Methodist Hospital in Fort Worth, Texas, two of their sons told NBC News.
The couple contracted the virus nearly a week before Thanksgiving. “It really took a toll on them pretty quickly,” son Shawn Blackwell said of his parents after they began exhibiting symptoms.
He said his mother was having shortness of breath at night and wasn’t sleeping. His father laid on the couch for four days. Their deteriorating conditions forced them to miss Thanksgiving with their children for the first time.
“There’s not been one Thanksgiving we’ve never spent together,” son Brandon Blackwell said.
The Friday after the holiday the couple was admitted to the hospital, where they’d spend the next few weeks fighting for their lives.
“It was hard to have them in the hospital,” Shawn Blackwell said.
The brothers weren’t able to physically see their parents and were only able to video chat with them. Their father broke down on one of those video calls, saying he didn't think he was going to make it.
“Their spirits were not too high during their hospital stay," Brandon Blackwell said. "But just us being there, I know, gave them some type of comfort. I was just glad they were able to see our faces.”
It was shortly after video calls with their children that the Blackwells were transferred to the intensive care unit.
“My little brother Shawn got to speak with my mom right before she got intubated and I was able to speak with my dad right before he got intubated, so it was crazy how that worked out,” Brandon Blackwell said.
The next time the sons would see their parents would be on their deathbeds.
“My dad wasn’t going to make it too much longer and my mom was right behind him,” Shawn Blackwell said. After consulting the doctors, the family made the difficult decision discontinue their life support.
Paul and Rosemary Blackwell died holding each other's hands — and the hands of Shawn and Brandon Blackwell, finally able to see their parents in person.
Strana storia, a dire il vero. Quindi sono morti perché gli hanno tolto il supporto vitale. Ma quando e perché l'hanno deciso? E come è accaduto che entrambi fossero nella stessa condizione? Mmmh, triste storia ma ripeto, molto strana.
Standing Rock Sioux elder who helped preserve Lakota language succumbs to Covid (nbcnews.com)
Standing Rock Sioux elder who helped preserve Lakota language succumbs to Covid
Jesse "Jay" Taken Alive, 65, was a former chairman of his tribe, an advocate for his people and a protector of the language and culture.
Jesse "Jay" Taken Alive died on Monday, Dec. 14, after contracting the coronavirus in October.Lakota Language Consortium
Dec. 17, 2020, 7:00 PM CET
By Erik Ortiz
In October, as the coronavirus outbreak swept across the Standing Rock Sioux Tribe's reservation, straddling the North and South Dakota border, tribal elder Jesse "Jay" Taken Alive was sidelined with a nagging cough.
He tested positive for Covid-19. Within a week, his wife, Cheryl, who was feeling congested and weak, did, too.
The couple's health began to deteriorate, their children recalled: Taken Alive was rushed to the Indian Health Service hospital in Fort Yates, North Dakota, and hospitalized for a few days. Later, he and his wife were both admitted to a larger hospital in Fargo, only one floor apart but unable to see each other.
Cheryl, a retired human services worker, could no longer walk on her own. She died on Nov. 11, at age 64.
Days later, doctors had suggested putting Taken Alive, whose lungs had declined, on a ventilator, according to his family. But Taken Alive resisted, retaining an upbeat spirit for his five adult children, 10 grandchildren and three great-grandchildren. (wow, aggiungo. A 65 anni già bisnonno)
On Monday, four of Taken Alive's children were with him in the hospital. He held their hands and spoke haltingly in his native Lakota language. "It's time," he told them. He was 65.
One of his sons, Ira Taken Alive, who had cared for his parents and was himself hospitalized with Covid-19 but recovered, said his father in recent days had come to grips with his failing health. But the loss of his wife — they would have been married 46 years next month — was especially cruel.
"In the end, if we could have listed the cause of death, we would have said he died of a broken heart," Ira Taken Alive said.
Jesse "Jay" and Cheryl Taken Alive were married for almost 46 years.
Ira Taken Alive followed in his father's footsteps in becoming an elected tribal leader, the vice chairman of the Standing Rock Sioux Tribe. The elder Taken Alive was chairman of the Standing Rock Sioux from 1993 to 1997 and a longtime council member before retiring in 2015.
Ira Taken Alive said his father was a fierce advocate for his people, recalling how he publicly called for the University of North Dakota to retire its Fighting Sioux nickname and logo in the 1990s, saying it did not honor their history and was the source of racist incidents for many years. The issue remained divisive, but the school eventually changed its mascot to the Fighting Hawks in 2015.
"When push came to shove, Standing Rock held its ground," Ira Taken Alive said.
Tracking coronavirus case surges in the United States
The list of issues his father was passionate about seemed never-ending: ensuring tribal sovereignty; speaking out against the taking of Indigenous lands by outside governments; solving the high drug abuse and suicide rates devastating tribal communities; providing access to higher education for young people; and supporting protests against the construction of the Dakota Access oil pipeline running within a half-mile of the Standing Rock Sioux Reservation.
On Thanksgiving Day in 2016, Taken Alive addressed hundreds of protesters at the Standing Rock High School in Fort Yates, and in an emotional speech that made some in the audience cry, he compared Native Americans joining forces at Standing Rock to the aiding of Sitting Bull at the Battle of the Little Bighorn in 1876.
"We must defend the women and children — and the water," he told the crowd.
Last year, Taken Alive was among the elders who welcomed the Swedish climate activist Greta Thunberg to the reservation during her tour of the United States. Taken Alive gave Thunberg a Lakota name: Maphiyata echiyatan hin win, translated to "woman who came from the heavens."
"Only somebody like that can wake up the world," he reportedly told Thunberg. "We stand with you. We appreciate you. We love you as a relative."
Maintaining the Lakota language and culture and sharing it with younger generations remained one of Taken Alive's biggest endeavors, said one of his daughters, Jessie Taken Alive-Rencountre.
Taken Alive worked with the nonprofit Lakota Language Consortium, which seeks to preserve the language, and taught it to schoolchildren in the McLaughlin School District in the Standing Rock Sioux Reservation. The children lovingly referred to Taken Alive as "LaLa Jay," meaning grandfather.
Taken Alive's family isn't certain how he and his wife contracted the coronavirus, but said the couple had been mindful of wearing masks and social distancing — even as many communities in the Dakotas outside of the reservation resisted mask mandates and saw a surge in cases this fall.
S.D. tribes say they're 'trapped in a house on fire' fighting Covid while governor lets it rage
The family is planning a virtual memorial service for the couple and a private burial next week.
"This virus has taken so many of our elders, so many of our treasures," Taken Alive-Rencountre said. "We think, how are we going to survive without my father's guidance and his teachings? But I realize after seeing all these posts and stories on social media from those who knew him, we're the ones who are going to have to keep what he taught us alive for future generations."
The loss of both her father and her mother, she said, "leaves a sense of emptiness, but also a sense of purpose."
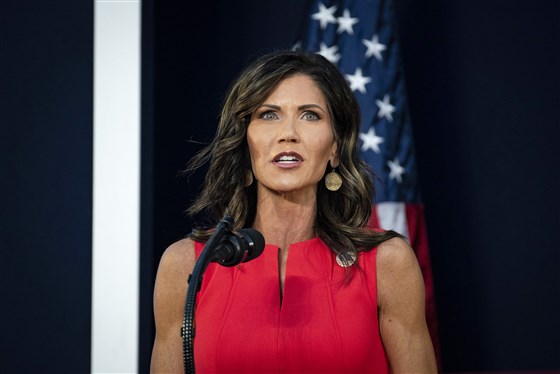
As South Dakota takes hands-off approach to coronavirus, Native Americans feel vulnerable (nbcnews.com)
As South Dakota takes hands-off approach to coronavirus, Native Americans feel vulnerable
"It's like we're trapped in a house on fire and we're doing our best to put it out," a member of the Cheyenne River Sioux Tribe said.
Nov. 25, 2020, 12:00 PM CET
By Erik Ortiz
In the early weeks of the pandemic, the Cheyenne River Sioux Tribe in South Dakota enacted drastic measures to fend off the spread of the coronavirus across its stark and sprawling prairie land.
The tribe installed checkpoints in April on roadways cutting through the Cheyenne River Sioux Indian Reservation to limit drivers without official business — part of a robust contact tracing program.
"We are doing this to save our residents, their lives," tribal Chairman Harold Frazier told NPR in May, when there was just one case of Covid-19 on the reservation, where about 12,000 people reside.
Even as case numbers stayed low, tribal officials imposed a mask mandate over the summer and rolled out mass testing events. And after South Dakota logged a record number of infections this month, Frazier on Monday began a 10-day lockdown of Eagle Butte, the remote town where the tribe's headquarters are located.
The efforts are in sharp contrast to how South Dakota Gov. Kristi Noem (Wow pensavo che fosse Melania Trump, le super-donne domineranno il mondo?) has overseen the pandemic in her state of nearly 885,000 residents.
Noem, a Republican, has avoided statewide mask mandates, lockdowns and the closing or restricting of businesses and churches. She said in a message last week that "we won't stop or discourage you from thanking God and spending time together this Thanksgiving" — a lenient message compared to those of the leaders of most other states, who have enforced curfews, stay-at-home orders and restrictions on indoor gatherings in the face of a surge in case numbers nationwide. (certo che i repubbli-cani non si smentiscono mai... ma proprio mai, eh).
Noem has also criticized the checkpoints set up by the Cheyenne River Sioux, as well as other Native American tribes in the state. In May, she asked the Trump administration to help intervene in a compromise to allow checkpoints on tribal roads but not state and federal ones within reservations.
Tribal members and other Indigenous-led groups in South Dakota say the lack of sweeping action — and the overt displays of opposition — on the part of state and some local officials stand to undermine their tribal sovereignty and attempts to protect their people during an intensifying public health crisis.
While the overall number of new Covid-19 infections has eased in recent days after it hit a record of more than 2,000 positive cases on Nov. 12, South Dakota this week still has among the highest rates of positivity and per capita deaths in the country, according to data from the Johns Hopkins Coronavirus Resource Center and the Centers for Disease Control and Prevention.
"It's like we're trapped in a house on fire, and we're doing our best to put it out," said Remi Bald Eagle, a Cheyenne River Sioux Tribe spokesman. "We see the firetrucks coming in the form of a vaccine, and we're wondering if it will get here in time before the fire burns us to death."
A disproportionate effect
The Cheyenne River Sioux Indian Reservation has had more than 1,100 cases of Covid-19, the disease caused by the coronavirus, with at least 13 deaths, tribal health officials say.
Statewide, Native Americans have been the hardest hit of any ethnic or racial group: While they make up only 9 percent of the population, they represent 14 percent of all cases and 15 percent of all deaths, according to Johns Hopkins' data.
Bald Eagle said many tribal members were previously diagnosed with underlying health conditions, such as diabetes and heart disease, and had limited access to health care on the reservation, which is partly in one of the most impoverished counties in the country.
The tribe has scrambled to set up makeshift beds and units, some of them in hotels and bingo halls, to supplement the eight hospital beds at the Cheyenne River Health Center, an Indian Health Services facility. The closest large hospitals, in Rapid City and in Bismarck, North Dakota, are two to three hours away, and health care professionals in South Dakota have warned of an overburdened health system.
A disturbing disconnect has also emerged among some patients. A South Dakota emergency room nurse's tweets went viral this month after she said she had encountered people dying of Covid-19 who didn't believe the virus was real.
Bald Eagle said tribes have a lot to lose if they ignore the science or take a hands-off approach, as the state has largely done.
"Some of those who died were our elders," he said. "They're some of our magnificent treasures. When they die, they take with them some of our language and our culture and our heritage, and we won't get that back."
The governor's office responded by referring to Noem's remarks at a news conference last week in which she encouraged hand-washing and social distancing.
"I've consistently said that people that want to wear masks should wear masks, and people that don't shouldn't be shamed because they choose not to," Noem said.
In a statement, the South Dakota State Medical Association said it supports a statewide mask mandate: "Masks work to decrease the risk of infection for everyone."
Checkpoint dispute
Tension has been escalating between tribes in South Dakota and Noem since the checkpoints went up.
In June, the Cheyenne River Sioux Tribe sued the federal government alleging that ever since Noem's plea for the White House's help, the Trump administration has abused its power by coercing the tribe to end its Covid-19 response plan, including its checkpoints.
The coercion included "threatening both monetary penalties and forcible dismantling of the Tribe's law enforcement program," the complaint alleges.
The Cheyenne River Sioux Tribe has set up nine health safety checkpoints along roads entering its reservation in South Dakota.Chairman Harold Frazier, Cheyenne River Sioux Tribe
Noem has said that South Dakota has rights that allow residents and travelers to access roadways and that the federal government has "an interest in interstate commerce," as well. But the tribe argues that it has jurisdictional powers over the state, and a 1990 appeals court ruling dictates that the state doesn't have control over roadways that cut through Native lands without tribal consent.
The lawsuit continues, and the tribe plans to respond in the coming days to the federal government's request to dismiss the case, said Nicole Ducheneaux, a tribal member and attorney. In the meantime, the tribe's nine checkpoints remain up.
"We are unspeakably vulnerable, and the state that surrounds us and the federal government that is supposed to protect us have decided to elevate a petty political agenda over human life," Ducheneaux said. "In the broader scheme of things, it was not so long ago that my people witnessed catastrophic disease and death that decimated our population, destabilized our society and almost wiped us out. If it were not for our sovereign powers of self-government, we would be at the mercy of Donald Trump and Kristi Noem, which would be a disaster of potentially existential proportions for our people."
A spokesman for the Interior Department, which is named in the suit, said tribal leaders had to follow federal regulations shared in early April about what steps to take to restrict access to or close roadways within reservations.
The federal government seeks to have the tribe's suit dismissed, in part because, it said, the checkpoints were operating with "unlawfully deputized individuals who did not have the required background investigations and/or basic police training."
The worsening pandemic has led other Native American groups in South Dakota to spar with local governments.
In October, police in Rapid City, the state's second-largest city, ordered the dismantling of an outdoor settlement — called Camp Mniluzahan — where Native Americans struggling with substance abuse and other hardships were provided shelter and food.
Police cited five of the volunteers, known as Creek Patrol, with obstruction and resisting arrest. A sixth person utilizing the camp was also cited. City officials said the camp was erected without proper permits in an area considered a flood zone. The camp has since moved from public property to land jointly owned by the Oglala, Rosebud and Cheyenne River Sioux tribes.
Rapid City Mayor Steve Allender said he didn't endorse the camp, and he hinted at the tensions last month.
"Every conversation about the homeless in the last month has been peppered with phrases like 'stolen land' and 'treaty violations' and 'getting land back' and that sort of thing," Allender said, according to NBC affiliate KNBN of Rapid City. "And so it appears that there's something much larger at hand than simply seeking shelter for the homeless."
Mark Tilsen, a Creek Patrol volunteer and member of the Oglala Lakota, said the lack of adequate social services or support from the local government underscores how Native Americans have historically had to cope with insufficient resources.
The camp's new location, which provides Covid-19 testing, helps 30 to 60 people daily, Tilsen said.
"We're essentially banding together to solve our problems as they come up," Tilsen said, crediting the efforts of previous generations of Native volunteers and activists. "We are lucky that we have found a way that the city cannot interfere with our work."
Natalie Stites Means, a director of the local Meals for Relatives program for Native American families affected by Covid-19 and a member of the Cheyenne River Sioux Tribe, said she worries that the disparate impact of the coronavirus on Indigenous communities is only going to worsen in the coming weeks because of lax attitudes. There is already a waiting list for families in need of food assistance, and Means counts on volunteers to help cook and transport meals.
"I'm not counting on Noem's administration to have the chops to do anything," Means said. "We're on our own.
COVID-19 as the Leading Cause of Death in the United States | Cardiology | JAMA | JAMA Network
COVID-19 as the Leading Cause of Death in the United States
December 17, 2020. doi:10.1001/jama.2020.24865
The current exponential increase in coronavirus disease 2019 (COVID-19) is reaching a calamitous scale in the United States, potentially overwhelming the health care system and causing substantial loss of life. The news media dutifully report each day’s increase in new cases and deaths, but putting these numbers in perspective may be difficult. The daily US mortality rate for COVID-19 deaths is equivalent to the September 11, 2001, attacks, which claimed 2988 lives,1 occurring every 1.5 days, or 15 Airbus 320 jetliners,2 each carrying 150 passengers, crashing every day.
A helpful approach to put the effects of the pandemic in context is to compare COVID-19–related mortality rates with the leading causes of death that, under ordinary circumstances, would pose the greatest threat to different age groups.3 The conditions listed in the Table include the 3 leading causes of death in each of the 10 age groups from infancy to old age. Using data from the Centers for Disease Control and Prevention, the Table shows mortality rates for these conditions during the period of March through October 20184 (the most recent year for which detailed cause-of-death data are available) with COVID-19 mortality rates during March through October 2020.5
Table. Age-Specific Mortality Rates (per Million) for COVID-19 (March-October 2020) and Other Leading Causes of Death (March-October 2018)a
View LargeDownload
The Table shows that by October 2020 COVID-19 had become the third leading cause of death for persons aged 45 through 84 years and the second leading cause of death for those aged 85 years or older. Adults 45 years or older were more likely to die from COVID-19 during those months than from chronic lower respiratory disease, transport accidents (eg, motor vehicle fatalities), drug overdoses, suicide, or homicide. In contrast, for individuals younger than age 45 years, other causes of death, such as drug overdoses, suicide, transport accidents, cancer, and homicide exceeded those from COVID-19.
Especially for older adults, the threat from COVID-19 may be even greater, for 3 reasons. First, the Table presents the aggregate 8-month mortality rate for COVID-19, not the current mortality rate, which has been increasing rapidly. Between November 1, 2020, and December 13, 2020, the 7-day moving average for daily COVID-19 deaths tripled, from 826 to 2430 deaths per day, and if this trend is unabated will soon surpass the daily rate observed at the height of the spring surge (2856 deaths per day on April 21, 2020).6 As occurred in the spring, COVID-19 has become the leading cause of death in the United States (daily mortality rates for heart disease and cancer, which for decades have been the 2 leading causes of death, are approximately 1700 and 1600 deaths per day, respectively4). With COVID-19 mortality rates now exceeding these thresholds, this infectious disease has become deadlier than heart disease and cancer, and its lethality may increase further as transmission increases with holiday travel and gatherings and with the intensified indoor exposure that winter brings.
Second, the reported number of COVID-19 deaths underestimates the excess deaths produced by the pandemic. Due to reporting delays and miscoding of COVID-19 deaths and an increase in non–COVID-19 deaths caused by disruptions produced by the pandemic, excess deaths are estimated to be 20% higher than publicly reported COVID-19 death counts.7 Third, COVID-19 is unlike other causes of death in the Table because it is communicable; individuals who die from homicide or cancer do not transmit the risk of morbidity or mortality to those nearby. Every COVID-19 death signals the possibility of more deaths among close contacts.
The failure of the public and its leaders to take adequate steps to prevent viral transmission has made the nation more vulnerable, allowing COVID-19 to become the leading cause of death in the United States, particularly among those aged 35 years or older. Much of this escalation was preventable, as is true for many deaths to come. The prospect of a vaccine offers hope for 2021, but that solution will not come soon enough to avoid catastrophic increases in COVID-19–related hospitalizations and deaths. The need for the entire population to take the disease seriously—notably to wear masks and maintain social distance—could not be more urgent.
LE CURE IGNORATE (da noi)
Covid, cure con idrossiclorochina: ok da Consiglio di Stato (adnkronos.com)
Covid, cure con idrossiclorochina: ok da Consiglio di Stato Pubblicato il: 11/12/2020 11:37
Il Consiglio di Stato dice sì all'uso dell'idrossiclorochina come terapia per Covid-19, purché sia prescritta da un medico, e conferma la decisione dell'Agenzia del farmaco di escludere il farmaco dalla rimborsabilità Ssn. Con l'ordinanza numero 7097/2020, pubblicata oggi, la III Sezione del Consiglio di Stato ha infatti accolto, in sede cautelare, il ricorso di un gruppo di medici di base e ha sospeso la nota del 22 luglio 2020 dell'Aifa che vietava la prescrizione off label (ossia per un uso non previsto dal bugiardino) dell'idrossiclorochina per la lotta al Covid 19.
"La perdurante incertezza circa l'efficacia terapeutica dell'idrossiclorochina, ammessa dalla stessa Aifa a giustificazione dell'ulteriore valutazione in studi clinici randomizzati - si legge nella corposa ordinanza - non è ragione sufficiente sul piano giuridico a giustificare l'irragionevole sospensione del suo utilizzo sul territorio nazionale da parte dei medici curanti".
E ancora: "La scelta se utilizzare o meno il farmaco, in una situazione di dubbio e di contrasto nella comunità scientifica, sulla base di dati clinici non univoci, circa la sua efficacia nel solo stadio iniziale della malattia, deve essere dunque rimessa all'autonomia decisionale e alla responsabilità del singolo medico in scienza e coscienza" e con l'ovvio consenso informato del singolo paziente, fermo restando il monitoraggio costante e attento del medico che lo ha prescritto.
L'ordinanza precisa che non è invece oggetto di sospensione (né a monte di contenzioso) la decisione dell'Aifa di escludere la prescrizione off label dell'idrossiclorochina dal regime di rimborsabilità.
MA C'E' DI PIU' E MOLTO PEGGIO.....
L'anticorpo monoclonale fatto in Italia che noi non usiamo. Prodotto a Latina, poteva curare (gratis) 10mila malati. I burocrati lo lasciano agli Usa - Il Fatto Quotidiano
L’anticorpo monoclonale fatto in Italia che noi non usiamo. Prodotto a Latina, poteva curare (gratis) 10mila malati. I burocrati lo lasciano agli Usa
Grazie alla terapia usata da Trump, 10mila nostri malati sarebbero potuti guarire. Ma il via libera alla sperimentazione è ancora in stallo. Clementi: "Abbiamo 'pallottole' che possono salvare migliaia di pazienti, ma decidiamo di non spararle"
di Thomas Mackinson | 17 DICEMBRE 2020
Diecimila italiani potevano guarire subito, come tanti Donald Trump. Invece, aspettando un vaccino, l’Italia va incontro alla terza ondata Covid senza terapie a base di anticorpi monoclonali, quelli che in tre giorni neutralizzano il virus evitando il ricovero. Da uno stabilimento di Latina in realtà escono furgoni carichi di questi farmaci, ma sono destinati a salvare pazienti americani, non gli italiani. Ai quali, per altro, erano stati offerti a titolo gratuito già due mesi fa. È il paradosso di una storia che ha pesanti risvolti sanitari, politici ed etici. “Abbiamo ‘pallottole’ specifiche contro il virus. Possono salvare migliaia di pazienti, evitare ricoveri e contagi, ma decidiamo di non spararle. Non si spiega”, ripete da giorni Massimo Clementi, virologo del San Raffaele di Milano.
Racconta che i colleghi negli Stati Uniti da alcune settimane somministrano gli anticorpi neutralizzanti come terapia e profilassi per malati Covid. La stessa cura che ha salvato la vita a Donald Trump in pochi giorni, nonostante l’età e il sovrappeso: “Dopo 2-3 giorni guariscono senza effetti collaterali apparenti”. Il tutto a 1000 euro circa per un trattamento completo, contro gli 850 euro di un ricovero giornaliero.
Gli Stati Uniti ne hanno acquistato 950mila dosi, seguiti da Canada e – notizia di ieri – Germania. Non l’Italia, dove si producono. Il nostro Paese ha investito su un monoclonale made in Italy promettente ma disponibile solo fra 4-6 mesi. Scienziati molto pragmatici si chiedono perché, nel frattempo, non si usino i farmaci che già si dimostrano efficaci altrove: fin da ottobre – si scopre ora – era stata data all’Italia la possibilità di usare questi anticorpi attraverso un cosiddetto “trial clinico”, nel quale 10mila dosi del farmaco sarebbero state proposte a titolo a gratuito. Una mano dal cielo misteriosamente respinta mentre il Paese precipitava nella seconda ondata.
Il farmaco – bamlanivimab o Cov555 – è stato sviluppato dalla multinazionale americana Eli Lilly. La sua efficacia nel ridurre carica virale, sintomi e rischio di ricovero è dimostrata da uno studio di Fase2 randomizzato (la fase 3 è in corso) condotto negli USA. I risultati sono stati illustrati sul prestigioso New England Journal of Medicine. Dall’headquarter di Sesto Fiorentino spiegano che l’anticorpo è stato messo in produzione prima ancora che finisse la sperimentazione perché fosse disponibile su scala globale il prima possibile.
Dal 9 novembre, quando l’FDA ne ha autorizzato l’uso di emergenza, gli Stati Uniti hanno acquistato quasi un milione di dosi. In Europa si aspetta il via libera dell’Ema che non autorizza medicinali in fase di sviluppo. Una direttiva europea del 2001 consente, però, ai singoli Paesi EU di procedere all’acquisto e la Germania ieri ha completato la procedura per autorizzarlo. A breve toccherà all’Ungheria. E l’Italia? Aspetta. Avendo il suo cuore europeo alle porte di Firenze, finito lo studio la società di Indianapolis ha preso contatto con le autorità sanitarie e politiche nazionali, anche italiane. Il 29 ottobre riunione con l’Aifa: collegati, tra gli altri, Gianni Rezza per il Ministero della Salute; Giuseppe Ippolito del Cts e direttore dello Spallanzani di Roma; il professor Guido Silvestri, virologo alla Emory University di Atlanta che aveva favorito il contatto con Eli Lilly. Sul tavolo, la possibilità di avviare in Italia la sperimentazione con almeno 10mila dosi gratis del farmaco che negli USA ha dimostrato di ridurre i rischi di ospedalizzazione dal 72 al 90%. In quel contesto viene anche chiarito che non sarebbe stato un favore alla multinazionale, al contrario: una volta che l’FDA l’avesse autorizzato, sarebbero partite richieste da altri Paesi.
L’occasione, da cogliere al volo, cade nel vuoto, forse per una rigida adesione alle regole di AIFA ed EMA che non hanno però fermato la rigorosa Germania. Altra ipotesi: l’offerta è stata lasciata cadere per una scelta già fatta a monte. Sui monoclonali da marzo il Governo ha investito 380 milioni per un progetto tutto italiano che fa capo alla fondazione Toscana Life Sciences (TLS), ente non profit di Siena, in collaborazione con lo Spallanzani e diretto dal luminare Rino Rappuoli. La sperimentazione clinica deve ancora partire e la produzione, salvo intoppi, inizierà solo a primavera 2021. A quanto risulta al Fatto, l’operazione con Eli Lilly, che già due mesi fa avrebbe permesso di salvare migliaia di persone, non sarebbe andata in porto per l’atteggiamento critico verso questi anticorpi del direttore dello Spallanzani che lavorerà al progetto senese. “Non so perché sia andata così, dovete chiedere ad AIFA”, taglia corto il direttore Giuseppe Ippolito, negando un conflitto di interessi: “Non prescrivo farmaci, mi occupo solo di scienza”.
Quando l’FDA autorizza il farmaco, la multinazionale non può più proporre il trial gratuito ma deve attenersi al prezzo della casa madre. Per assurdo, sfumata l’opzione a costo zero, l’Italia esprime una manifestazione ufficiale di interesse all’acquisto. Il negoziato va in scena il 16 novembre alla presenza di Arcuri, del DG dell’Aifa Magrini e del ministro della Salute Speranza. Si parla di prezzo e di dosi ma il negoziato si ferma lì e non va avanti. Neppure quando il sindaco di Firenze torna alla carica. Dario Nardella annuncia ai giornali di aver parlato coi vertici di Eli Lilly e che “se c’è l’ok della Commissione Ue, la distribuzione del farmaco a base di anticorpi monoclonali potrebbe cominciare dopo Natale non solo in Francia, Spagna e Regno Unito ma anche in Italia”. Natale è alle porte e in Italia non c’è traccia di farmaci anticorpali né si ha notizia di una pressione dell’Aifa per sollecitare l’omologa agenzia europea. Come se l’opzione terapeutica per pazienti in lotta col virus, già disponibile altrove, non interessasse.
L’AIFA e la struttura di Arcuri – sentite dal Fatto – ribadiscono: finché non c’è l’autorizzazione EMA non si va avanti. Di troppa prudenza si può anche morire, rispondono gli scienziati. “Io avrei accelerato”, dice chiaro e tondo il consulente del ministro Walter Ricciardi, presente alla riunione un mese fa: “Con tanti morti e ospedalizzati valutare presto tutte le terapie disponibili è un imperativo etico e morale”. Il virologo Silvestri, che tanto aveva spinto: “Non capisco cosa stia bloccando l’introduzione degli anticorpi di Lilly e/o Regeneron, che qui negli States usiamo con risultati molto incoraggianti”. Ieri sera si è aggiunta anche la voce critica dell’immunologa dell’università di Padova Antonella Viola: “E’ sorprendente questo ritardo, cosa aspettiamo?”.
Per il professor Clementi, siamo al paradosso. “È importante trovare il miglior farmaco possibile, ma non possiamo scartare a priori una possibilità terapeutica che altrove salva le persone. Una fiala costa poco più di un giorno di ricovero e ogni risorsa che risparmi la puoi usare per altro. Tenere nel fodero un’arma che si dimostra decisiva è incomprensibile. Da qui, la mia sollecitazione all’AIFA”.
Certo, una soluzione al 100% italiana garantirebbe autosufficienza e prelazione nell’approvvigionamento. Da Sesto Fiorentino, però, rispondono che il loro farmaco, oltre ai benefici in termini di salute e risparmio, avrebbe avuto anche ricadute economiche per l’Italia: nella produzione è coinvolto un fornitore italiano, la Latina BSP Pharmaceutical. “Se andrà bene potremmo distribuirlo non solo negli Usa ma anche in Italia”, esultava a marzo il titolare dell’impresa pontina, Aldo Braca. Nove mesi dopo dallo stabilimento di Latina esce il farmaco più promettente contro il Covid. Ma va soltanto all’estero.
Articolo aggiornato il 17 novembre
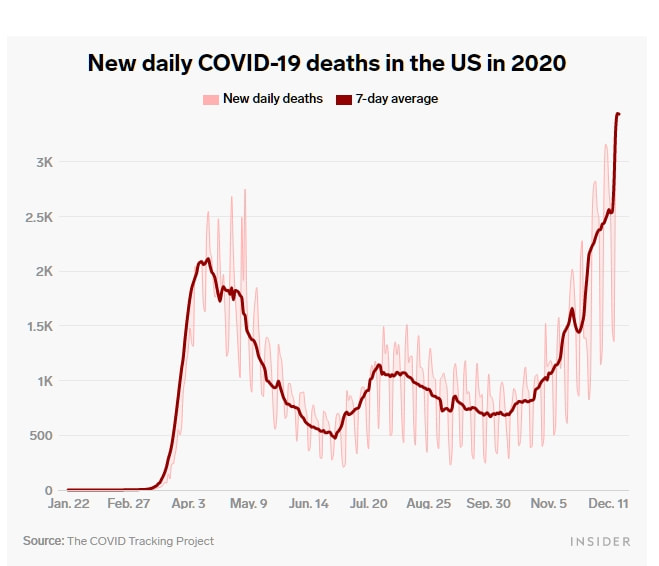 |  |

{kind=link}