4-12-20:
Oramai la parola d'ordine sembra essere 'arrivano i vaccini, torniamo a vivere e lasciamoci quest'anno orrendo alle spalle'.
Del resto, lo capisco anche, visti i danni e le perdite che abbiamo subito.
Ma come pensare seriamente che la via intrapresa sia quella giusta?
Specie se ci si dimentica così facilmente del... passato?
Questa seconda ondata ci ha massacrati e il bello è, anche se non possiamo ammetterlo più di tanto, che continuerà a farlo anche in futuro. Alla fine sarà il COVIDDI' a vaccinarci in un modo, o in un altro.
Ecco perché ce l'ho con tutta quella marmaglia che ha negato l'evidenza del fenomeno, da Montanari a Salvini, dalla Confindustria ai dottoroni televisivi: gente come Bassetti, come Zangrillo, da ultimo Palù, che ha bacchettato Crisanti ma sul suo ruolo per salvare il Veneto o qualsiasi altra cosa, non è dato sapere molto.
E poi ci sono quei bellimbusti alla Bacco, quello che 'uccidono i pazienti con terapie sbagliate' oppure quell'altro soggettone di Resta, quello che 'il COVID ha ucciso meno dello 0,1% della popolazione' (ed è un dottore pure lui, eh). Scoglio (quello che 'ha smentito l'ISTAT', però non sa nemmeno leggere i suoi rapporti fino a pagina 6). E così via.
E peggio ancora, per me, gente come Guarino, che di sponda con altri 'giornalisti' ha la pretesa di fare controinformazione, con frasi illuminanti sul tipo: 'controinformazione: oggi guariti 1000, ricoverati 140'.
Gentaglia che ha passato l'estate a parlare di allarmismo, di libertà, di economia, di 'vita' (quale?) e accusato il governo Conte di fare 'terrorismo'.
Tutti loro hanno le loro ragioni e i loro torti. La verità non è semplice. MA se devi accusare il governo Conte di qualcosa, dovresti partire da quel che è successo a Bergamo. E sopratutto, non dovresti dimenticarti di Fontana, Gallera e Confindustria. E di Renzi, che all'epoca (ma questo l'articolo del NYT non lo ricorda) stava sempre con il fiato sul collo di Conte, sempre pronto alla 'resa dei Conti' (sic). Questo fino ad inizio marzo. Poi da giugno Salvini e Meloni, più quell'altro pazzoide del generale Pappalardo, in giro per le piazze a manifestare contro il governo, come se la chiusura l'avessero fatta apposta, e non obtorto collo nonostante Confindustria volesse il contrario, perché a Bergamo 'siamo sempre aperti'.
Strano poi, come a questi soggetti, tutti quelli sopra, non sia preso nulla durante l'epidemia. Nemmeno un raffreddorino. Tanto meno il COVID, come ha beccato Berlu e Johnson, e pure Trump e forse Bolsonazista.
Strano, sì, ma purtroppo NON comune. In un solo mese il resto d'Italia ha avuto 12.000 morti. Dall'inizio di ottobre siamo a +23.000. L'altro giorno siamo arrivati (il 3-12) al nuovo 'record'. 993. Anche se pare che parte di essi fossero dei giorni precedenti, sempre morti sono.
E questo in un paese dove alle volte non riescono nemmeno a seppellire i morti (vedi Palermo, che pure non ha avuto tutto 'sto Covid).
Insomma, ce ne sarebbero tante da dire, ma pensare che l'estate l'abbiamo passata a darci le pacche sulle spalle che il coviddi non c'era più, a pensare ai monopattini, ai banchi con le rotelle e così via... incredibile veramente.
E d'autunno non abbiamo imparato niente.
In Umbria, Perugia ha avuto un incremento di mortalità che nella prima ondata non solo non esisteva, ma era addirittura tra le città con mortalità negativa rispetto alla media normale (e se è per questo, pure Palermo...).
E adesso abbiamo i morti anche lì, dottori di 62 anni, sbandieratori di 45... e così via.
Perugia: mortalità 1-15 novembre +66% (98 vs 58) = 39 morti in più, ma i morti per COVID ufficialmente sono stati solo 26. Perugià è l'8a tra le città per aumento % della mortalità.
A ottobre le cose erano andate meglio: 160 decessi, contro una media 135 = +19%
Nel periodo 30-9 ----17/11: 270
20 -- 0-64 anni
28 -- 65-74 anni
79 -- 75-84 anni
143 -- 85+ anni
Tra le vittime anche un dottore di 62 anni.
Nel resto del mondo le cose non vanno poi così bene: siamo arrivati a oltre 200.000 casi negli USA, 680.000 in tutto il mondo, con 3.000 morti americani al giorno, e oltre 12.000 nel mondo intero.
E meno male che Palù non considera il COVID una 'pandemia', per agioni che l'eccelso scenziato non ha spiegato bene.
Dunque, cominciamo da una definizione che dovrebbe essere chiara, ma che non lo è, nonostante nove mesi di disastri.
Per tutti quelli che dicono 'è un'influenzetta', ecco un elemento che dovrebberos studiarsi per bene:
www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-disease-2019-vs-the-flu
Coronavirus vs. Flu DeathsCOVID-19: There have been approximately 1,509,141 deaths reported worldwide. In the U.S, 276,401 people have died of COVID-19 between January 2020 and December 4, 2020.*
Flu: The World Health Organization estimates that 290,000 to 650,000 people die of flu-related causes every year worldwide.
The COVID-19 situation is changing rapidly. Since this disease is caused by a new virus, the vast majority of people do not yet have immunity to it, and a vaccine may be many months away. Doctors and scientists are working to estimate the mortality rate of COVID-19, but at present, it is thought to be substantially higher (possibly 10 times or more) than that of most strains of the flu.
www.fanpage.it/attualita/quanto-sono-aumentati-i-decessi-in-italia-nel-2020-a-causa-del-coronavirus/
L'Istat calcola l’aumento dei decessi a marzo
I dati più rilevanti sono quelli di marzo, con la stima dell’eccesso di mortalità nel 2020 rispetto alla media degli anni precedenti. I dati consolidati mostrano che la mortalità in eccesso in Italia in quel mese è del 47,2%. Un dato che deriva soprattutto dall’impatto al Nord, dove la mortalità in eccesso è del 93,9%. Al Centro, invece, la quota riguardante i decessi in eccesso è del 12,2%. Al Sud l’impatto è invece minore, con un +4,3% rispetto alla media degli anni precedenti.
I decessi totali in Italia nel 2020
I decessi in Italia a marzo sono stati 86mila, con un calo progressivo nei mesi successivi: 73mila ad aprile, 52mila a maggio, 48mila a giugno. Poi una leggera risalita in estate, con 50mila decessi a luglio e 51mila ad agosto. Il totale dei decessi in Italia da gennaio ad agosto è di 475mila morti, di cui ben 243mila al Nord, 143mila al Mezzogiorno e 89mila al Centro Italia.
L’aumento della mortalità a causa del Coronavirus
L’Istat segnala come nei primi due mesi del 2020 ci fosse una diminuzione ella mortalità praticamente in tutte le Regioni, con un dato totale italiano al -7,3%. Ma a marzo la situazione è cambiata radicalmente: l’aumento dei decessi è del 47,2%. Ad aprile, ancora, è del 39,2%. Un dato che dipende soprattutto dai decessi registrati al Nord, con un +74,3%, mentre al Centro l’aumento è del 12,6% e al Sud del 6,8%. A maggio, dopo il lockdown, il numero di decessi totali al Centro e al Sud è diminuito, con un aumento che invece si registra solo al Nord (+7,2%): in Italia alla fine a maggio si ha un +2,1% dei decessi rispetto agli anni precedenti.
In estate la situazione cambia: a giugno in Italia i decessi diminuiscono dell’1,5%, con un decremento più netto al Centro e al Sud. A luglio, invece, le morti registrate sono di meno soprattutto al Nord e il dato nazionale è in calo del 3% rispetto agli anni precedenti. Si registra di nuovo un leggero aumento ad agosto, soprattutto al Centro e al Sud. Il totale dei morti registrati in Italia da gennaio ad agosto è in aumento dell’8,6% rispetto alla media 2015-2019. Al Nord questo aumento è molto marcato: +19,5%. Al Centro (-0,2%) e al Sud (-1,1%) i decessi sono invece in diminuzione nel 2020, nonostante il Covid.
Infine, l’Istat fornisce anche i dati riguardanti le singole Regioni mese per mese. Il tasso di mortalità in Lombardia è in aumento a marzo addirittura del 191,2% rispetto all’anno precedente, a dimostrazione dell’impatto del Covid. Un dato che poi scende al 117% ad aprile, ma prima di tornare a livelli simili a quelli degli anni precedenti bisogna aspettare fino all’estate. L’aumento dei decessi rispetto agli anni precedenti è molto alto anche in altre Regioni, come Emilia-Romagna, Trentino-Alto Adige, Piemonte, Liguria e Valle d’Aosta. Tutte Regioni del Nord.
www.globalist.it/science/2020/11/29/il-rianimatore-con-52-mila-morti-di-covid-e-intollerabile-il-dibattito-sulle-cene-di-natale
Il rianimatore: "Con 52 mila morti di Covid è intollerabile il dibattito sulle cene di Natale"
Massimo Antonelli, direttore della terapia intensiva del Policlinico Gemelli, componente del Cts. "Negazionisti ne ho curati molti, una volta guariti si scusano"
globalist
29 novembre 2020
Molti se non toccano con mano non credono, E perfino alcuni non credono a quello che sta loro accadendo. Sono i negazionisti.
"Il dibattito sul sì a veglioni e cene di Natale? Per me, per tutti i colleghi, è intollerabile, pur condividendo le ansie degli operatori che vedono sfumare altre opportunità economiche. In Italia le vittime del Covid sono state circa 52mila. Ogni giorno qui ne vediamo andar via almeno 70. E c'è chi non vuole rinunciare, per una sola volta nelle vita, a occasioni superflue".
Parola di Massimo Antonelli, direttore della terapia intensiva del Policlinico Gemelli, componente del Cts
“La frustrazione più grande? Non poter essere visto da chi ci guarda dal letto, ed è solo. Dover comunicare soltanto con gli occhi. I nostri morti meritano rispetto. Che senso avrebbe un Natale come se niente fosse o andare sulla neve? Tante persone tendono a porre l'accento sugli aspetti economici e le difficoltà degli esercizi commerciali. Comprendo. Tante altre invece perdono inconsciamente la percezione di una situazione drammatica. I negazionisti? Ne abbiamo curati tanti al Gemelli. Una volta fuori, si sono scusati. Professore, le prometto che farò di tutto per aiutarvi".
Antonelli è d'accordo quindi con le restrizioni. "E come non potrei? I numeri parlano. Oltre alla mortalità, l'incidenza dei nuovi casi resta alta, siamo oltre 320 su 100 mila abitanti. Alcune regioni superano i 700-800 casi al giorno. È vero la curva rallenta, l'Rt è sceso sotto l'unità. Però...allentare significa andare incontro a una terza ondata. Non è un rischio. È una certezza".
MA vi siete mai chiesti come e quando conteggiano i decessi da COVID? Io spesso. Ecco quel che rispondono dal Veneto.
www.ilfattoquotidiano.it/2020/11/27/coronavirus-in-veneto-i-decessi-in-terapia-intensiva-sono-il-14-del-totale-il-primario-ecco-perche-si-muore-soprattutto-nei-reparti/6018246/
Coronavirus, in Veneto i decessi in terapia intensiva sono il 14% del totale.
Il primario: “Ecco perché si muore soprattutto nei reparti”
I dati presentati dalla Regione, relativi alle vittime dal 21 febbraio al 17 novembre, analizzati dal dottor Ivo Tiberio, primario di terapia intensiva dell'ospedale di Padova: "La risposta è difficile, perché ogni ospedale ha la propria organizzazione assistenziale e bisognerebbe verificare le motivazioni per cui i deceduti erano in altri reparti. La spiegazione più ovvia è che non potessero migliorare anche se curati nell'unità critica, che l'accanimento fosse ormai inutile o che fossero giù curati con ossigenoterapia e ventilatori in altri reparti"
di Giuseppe Pietrobelli | 27 NOVEMBRE 2020
Perché più di metà dei decessi da Covid avvengono in ospedale, ma non nei reparti di terapia intensiva, bensì in Malattie infettive o Pneumologia? La domanda è posta, implicitamente, dai dati che il governatore del Veneto, Luca Zaia, ha fornito alla stampa, per rappresentare il quadro delle vittime che si sono registrate in regione dal 21 febbraio al 17 novembre. La terapia intensiva sembrerebbe essere l’ultima spiaggia dove si affronta lo scontro con la malattia. Ma non è così. L’elenco totale riguarda 3.056 persone. Di queste, ne sono deceduti in area critica 434, pari al 14,2 per cento. Molti di più sono quelli che si trovavano in altri reparti Covid: 1.719, pari al 56%. Praticamente una persona su due che poi non ce la farà, finisce all’ospedale, ma non in terapia intensiva. O perlomeno non è lì che avviene la morte. Il 23 per cento (698) sono invece deceduti nelle residenze per anziani, i restanti 465 a domicilio.
“Non pensiate che questi ultimi ce li siamo dimenticati a casa”, ha spiegato Zaia per allontanare il sospetto che il sistema sanitario abbia sottovalutato i sintomi. Si è trattato di una scelta dei medici, dettata dalle condizioni dei pazienti. Ma perché i decessi in terapia intensiva raggiungono appena un settimo del totale e un quarto di quelli avvenuti in altri reparti Covid? L’interrogativo è cruciale perché riguarda il modo con cui un paziente viene curato. Il dottor Ivo Tiberio, primario di terapia intensiva dell’ospedale di Padova, è responsabile delle unità critiche sia del nosocomio di via Giustiniani che nell’ospedale Sant’Antonio, ognuna con 18 letti. E spiega: “La domanda è corretta, ma la risposta è difficile, perché ogni ospedale ha la propria organizzazione assistenziale e bisognerebbe verificare le motivazioni per cui i deceduti erano in altri reparti. La spiegazione più ovvia è che non potessero migliorare anche se curati nell’unità critica, che l’accanimento fosse ormai inutile o che fossero giù curati con ossigenoterapia e ventilatori in altri reparti”.
Ma come si fa a stabilire qual è il trattamento più adeguato? “In via generale si seguono quattro criteri: la gravità della patologia di cui soffre il paziente; poi la cormobilità, ovvero la presenza di altre patologie; in terzo luogo il tempo di risposta al trattamento, che in genere è più breve se il paziente è più giovane, visto che reagisce meglio; infine, l’età”. Quindi gli anziani vengono ricoverati di meno in terapia intensiva? “L’età da sola non è un criterio per includere o escludere dalle unità critiche, però a seconda dell’età variano anche le possibilità di sopravvivenza”.
Non è un criterio assoluto, spiega il dottor Tiberio, ma una combinazione di elementi. “L’età è un fattore di rischio. Ma io ho intubato ed estubato un paziente di 86 anni. Quindi bisogna considerare la risposta del malato ai trattamenti”. Nei due reparti padovani il primario ha registrato una mortalità del 18 per cento durante la prima ondata, del 7-8 per cento nella recrudescenza più recente. “Valuto che ci si assesterà su una media del 12-13 per cento. L’andamento del secondo periodo è stato diverso da quello primaverile e da noi è cominciato il 4 luglio con un primo di caso di un uomo di 57 anni. Inizialmente, d’estate, hanno cominciato ad arrivare persone più giovani – quarantenni e cinquantenni – perché hanno una vita di relazione sociale più intensa degli anziani”. Ed è per questo, secondo il primario, che “il tasso di mortalità dopo la seconda esplosione è stato più basso del primo”. Il contagio, sempre secondo Tiberio, è da ricondurre anche agli spostamenti estivi. “Ma adesso l’età dei ricoverati si sta alzando, quindi prevediamo che cresca anche la percentuale di decessi in terapia intensiva. E non dimentichiamo che non sempre è facile attribuire la causa della morte al Covid o ad altre patologie, respiratorie o cardiopatiche”.
CONVINCENTE? MAH! A me non pare molto... voglio dire, persino adesso, con le T.I. NON pienate a tappo, i morti nelle RSA sono quasi il doppio di quelli nelle T.I.? E come li hanno curati in quei casi? E i 465 a 'domicilio', come si spiegano?
Per me non si spiegano proprio. Scusate, ma no. Se uno sta male, è giusto portarlo in ospedale e se c'é la T.I. è giusto usarla. Come mai le T.I. risultano vuote per oltre il 50% e i pazienti crepano a domicilio? Ma che senso ha?
Ma c'é di PEGGIO in termini di gestione dei pazienti? Beh, per esempio andando a Taranto. A BALLARE IN PUGLIA, come direbbe Caparezza.
www.ilgiorno.it/bergamo/cronaca/coronavirus-new-york-morti
Coronavirus, errori e ritardi: la strage di Bergamo sul New York Times
Un'inchiesta ripercorre le indecisioni che hanno fatto pagare il prezzo più alto a questa provincia durante la prima ondata della pandemia
Bergamo, 29 novembre 2020 - "Uno dei più letali campi di sterminio del mondo occidentale". Così il New York Times definisce Bergamo, all'interno di un'ampia inchiesta dedicata alle conseguenze del coronavirus in una delle zone più colpite dalla pandemia duranta la prima ondata.
"I giorni perduti che hanno reso Bergamo una tragedia del coronavirus" è il titolo del servizio giornalistico pubblicato sul giornate statunitense, che analizza "errori di gestione e ritardi burocratici hanno reso il bilancio molto peggiore di quel che doveva essere", si legge nell'articolo. Il giornale ripercorre nel dettaglio, anche con interviste, le drammatiche tappe della diffusione dell'epidemia, fin dai primi giorni quando le indicazioni erano di sottoporrre a esami solo "chi aveva legami con la Cina".
Solo il 20 febbraio - ricostruisce il New York Times - Annalisa Malara, medico di Codogno, decise di "rompere il protocollo" e "testare un uomo che mostrava una polmonite che non rispondeva alle cure standard": l'uomo sarebbe diventato il paziente zero, il primo caso accertato di Covid 19 in Italia.
L'inchiesta ricorda gli errori commessi nella gestione sanitaria e il contrasto tra governo centrale ed autorità locali, che generarono "dieci giorni di indecisione", con scelte che dovevano essere fatte ma non lo furono. E quando "l'Italia ha bloccato l'intera Regione e poi l'intero Paese, Bergamo era persa"
Spesso anche d'estate mi chiedevo: ma se ci sono solo 40 ricoverati in T.I. come è che ogni giorno ci sono 3-10 morti? Boh. Anche leggere quest'articolo del FQ non ha aiutato i suoi lettori ad avere idee più chiare:
www.nytimes.com/2020/11/29/world/europe/coronavirus-bergamo-italy.html
THE LOST DAYS THAT MADE BERGAMO A CORONAVIRUS TRAGEDY
The northern Italian province became one of the deadliest killing fields for the virus in the Western world. But a Times investigation found that faulty guidance and bureaucratic delays rendered the toll far worse than it had to be.
BERGAMO, Italy — When Franco Orlandi, a usually hale former truck driver, arrived in mid-February with a cough and fever at an emergency room in the northern Italian province of Bergamo, doctors determined that he had a flu and sent him home. Two days later, an ambulance brought the 83-year-old back. He couldn’t breathe.
Italy had not recorded a single domestic coronavirus case, but Mr. Orlandi’s symptoms puzzled Monica Avogadri, the 55-year-old anesthesiologist who treated him at Pesenti Fenaroli Hospital. She didn’t test him for the virus because Italian protocols, adopted from the World Health Organization, recommended testing only people with a link to China, where the outbreak had originated.
When she asked whether Mr. Orlandi had a connection to China, his wife seemed befuddled. They hardly ever ventured beyond their local cafe, Patty’s Bar.
‘‘China?” Dr. Avogadri recalled Mr. Orlandi’s wife responding. “She didn’t even know where it was.”
What Dr. Avogadri did not know was that Covid-19 had already arrived in her region of Lombardy, a discovery made five days later by another doctor in nearby Lodi who broke the national testing protocol. By then, Dr. Avogadri, hamstrung by those same protocols, had herself fallen ill after days caring for Mr. Orlandi and other patients. Her hospital, rather than identifying and treating the disease, was accelerating its spread across Italy’s economic heartland.
Bergamo became one of the deadliest killing fields for the virus in the Western world, a place marked by inconceivable suffering and a dreadful soundtrack of ambulance sirens as emergency medical workers peeled parents away from children, husbands from wives, grandparents from their families.
Hospitals became makeshift morgues and produced parades of coffins and scenes of devastation that became a warning to officials in other Western countries of how the virus could rapidly overwhelm health systems and turn infirmaries into incubators.
Officials confirmed that more than 3,300 people died with the virus in Bergamo, though they said the actual toll was probably double that. Mr. Orlandi’s town, Nembro, became perhaps Italy’s hardest struck, with an 850 percent increase in deaths in March. So many, the local priest ordered a stop to the incessant tolling of the bells for the dead.
The question of how such a tragedy could unfold in Bergamo, a wealthy, well-educated province of just more than a million, with top-level hospitals, has remained an uneasy mystery, a blood stain that the government prefers to avoid as it points with pride to Italy’s success in flattening the first wave of infections.
Unchecked, the virus spread everywhere. At one Bergamo nursing home, 34 of 87 guests died.
The World Health Organization’s guidance on testing engendered a misplaced sense of security and helped blind doctors to the spread of the virus. But missteps and inaction after Covid-19 exploded into view aggravated the situation and cost Bergamo — and Italy — precious time when minutes mattered most.
The director of Pesenti Fenaroli Hospital closed its doors almost as soon as he realized he had an outbreak. But regional officials ordered them opened hours later. Hospital workers, visitors and discharged patients were exposed to the virus, and then moved through the province.
For days, there was an expectation that the national government would lock down towns in Bergamo, as it had earlier done immediately and decisively in Lodi. Some mayors in Bergamo waited anxiously for the police to seal the borders, even as many business and local leaders expressed reluctance.
Italy’s prime minister, Giuseppe Conte, publicly turned to a committee of scientific advisers, which formally proposed that he follow the example of Lodi and shut down the newly infected towns in Bergamo. Privately, though, national business lobbies urged him not to close the area’s factories.
Ultimately, after critical days filled with bureaucratic dithering, as well as spats between Rome and the regional authorities, the government decided the time to save Bergamo had passed.
With the virus out of control in the province and clusters emerging all around it, the government waited longer but then went bigger. Two weeks after Mr. Orlandi had tested positive, Italy locked down the whole region. Then the country. But Bergamo was lost.
Misdirected Doctors
Now that the coronavirus, deep into its second wave, has washed across the globe and left virtually no nation untouched, it is easy to forget how alone among Western democracies Italy was in February, confronted with a threat for which it had no playbook.
Throughout flu season, some local family doctors in the Lombardy region had noticed strange pneumonia cases and were prescribing more scans than usual. The region has business ties to China, and local infectious disease doctors had kept an eye on the coronavirus outbreak in the city of Wuhan. They also trusted Italy’s new and narrower protocols, adopted from the W.H.O. at the end of January, which essentially limited testing to people linked to China.
But hardly any of the pneumonia patients had such a link, which meant that the few people being tested were mostly air travelers. All had come back negative.
Then, on Feb. 20, Annalisa Malara, a doctor in the town of Codogno, in Lodi province, decided to break the protocol and test a 38-year-old man with serious pneumonia who was not responding to standard treatments. The man’s test came back positive that same evening and he became Italy’s first known locally transmitted case of Covid-19.
Two days later, on the outskirts of Rome, an emergency meeting was held at Italy’s Civil Protection Agency, the national disaster relief body. Crammed into a small conference room, Mr. Conte sat at the head of an oval table, surrounded by his ministers, as Italy’s health minister, Roberto Speranza, proposed a dramatic lockdown of towns in the Lodi area.
The ministers, exchanging nervous looks, unanimously agreed and the government dispatched Italy’s police and army to seal the borders on Feb. 23 — a decision that it cites to this day as the metric of its boldness and willingness to put Italy’s public health over its economy.
Mr. Speranza weighed the momentous decision carefully, deciding it was better to err on the side of caution.
‘‘I was playing with the lives of people,” he said, adding that in the story of the pandemic, “It was the first time in the history of Western countries that we were locking down and taking away the freedom of the people.”
‘We Were Screwed’
The discovery of the virus in Lodi, just 60 miles from Bergamo, struck Dr. Avogadri, sick in bed at home, with the force of a revelation.
She picked up the phone on Feb. 21 and called her colleagues at Pesenti Fenaroli, in the town of Alzano Lombardo in Bergamo’s industrial and densely populated Serio river valley. She urged them to test her patient, Mr. Orlandi.
At first, they ridiculed her, noting that he’d never been anywhere near China. But other patients on the same floor were deteriorating, and another man with suspicious symptoms soon arrived in the emergency room. Hospital officials decided to swab test him and one of Mr. Orlandi’s roommates.
By midday on Feb. 23, the results were brought to Dr. Giuseppe Marzulli, the hospital director. Both tests were positive.
Dr. Marzulli grilled the reporting doctor about whether the staff had adequately investigated connections to China. They had. There weren’t any. The virus was already circulating in their midst.
“It was at that moment I understood we were screwed,” Dr. Marzulli said. “We had looked for who had been in China, and this was the tragic error.”
They swabbed Mr. Orlandi that day, as members of his family moved through crowded corridors of the third floor.
Some visitors noticed staff members coughing.
Red Cross workers helping a patient in Pradalunga, another area in the Serio river valley, in March.
Dr. Giuseppe Marzulli, the former director of the Pesenti Fenaroli hospital, tried to shut its emergency room after finding cases in late February. He was swiftly ordered to reopen.
Given the government’s swift action in Lodi, Dr. Marzulli began to prepare for a lockdown. He canceled shift changes so that no new personnel would come in, and he closed the emergency room, mindful that the hospital had only about a dozen swabs to perform coronavirus tests.
“We didn’t have swabs. It was the biggest problem we had,” he said.
Hours later, the region and the Bergamo hospital network overseeing Pesenti Fenaroli decided together to reopen the emergency room over Dr. Marzulli’s objections.
Aida Andreassi, a senior Lombardy health official, said the emergency room had been sanitized and the hospital represented an “indispensable garrison” for a region that needed all its medical facilities.
But without enough swabs, Dr. Marzulli said, the hospital was defenseless.
On Feb. 24, Mr. Orlandi’s test results came back. He was positive, too. By then, about 50 more patients had arrived at the emergency room with symptoms, quickly burning through the hospital’s stock of swabs, Dr. Marzulli said.
A doctor, who tested Dr. Avogadri with one of the available swabs, pressed hospital officials for more tests, reminding them in a frantic email that they had “symptomatic colleagues who have not been swabbed.”
His superiors pleaded with another hospital in the region for 100 swabs, according to email correspondence seen by The New York Times. But Dr. Marzulli said only half of them made it to Pesenti Fenaroli, on Feb. 26.
He scrambled, separating patients with symptoms from those without, and sending home visibly sick staff members. But many patients who came in contact with the virus stayed put, while their nurses and doctors kept circulating.
On Feb. 27, documents provided by Lombardy show, the region sent hundreds more swabs to the Bergamo hospitals. But they didn’t arrive at Pesenti Fenaroli right away, Dr. Marzulli said.
He was forced to ration out a couple dozen swabs a day until March 1, when he himself fainted from exhaustion with the virus.
“If we have to identify a spark,” Giorgio Gori, the mayor of Bergamo city said as infections devastated his town, “it was the hospital.”
Ten Days of Indecision
The small towns around the hospital increasingly became central to a drama playing out between Bergamo and Rome.
On Feb. 25, Bergamo province reported just 18 cases compared to 125 in Lodi. Lombardy’s top health official expressed concern about contagion at Pesenti Fenaroli Hospital but said, “It’s early to say if it’s another cluster.”
In Rome, Mr. Conte discouraged expanding testing, reasoning that health officials had to follow international protocols, “otherwise we would end up dramatizing” the emergency.
On Feb. 26, with 20 reported cases in Bergamo, Rome’s scientific committee said it didn’t see any flare-ups that required a lockdown. Claudio Cancelli, the mayor of Nembro, said Bergamo’s health officials threatened to cut off funding to the area’s 18 mayors if they closed centers for the elderly or disabled.
The next day, he said, they assured the mayors, “Don’t worry. There is no red zone foreseen.”
But on Feb. 28, Bergamo’s caseload had jumped to 103, against 182 in Lodi. At a Lombardy regional news conference, leading doctors identified the Pesenti Fenaroli Hospital as the outbreak’s source.
Confindustria Bergamo, the province’s industrial association, responded that same day by posting a video titled, “Bergamo Is Running.”
“Current health warnings from Italian government officials are that the risk of infection is low,” the narrator stated. The images showed factories humming.
That message resonated with Simona Ghilardi, who ran a national transport and logistics company in Nembro, about a mile from Pesenti Fenaroli Hospital. Colleagues in locked-down Lodi had told her about losing clients. Stopping industry in Bergamo was unthinkable to her.
“When you are born here the first thing they tell you is — you have to work,” she said.
Industrial leaders in Bergamo province lobbied the government not to close factories.
Despite the concerns of industry, government leaders said they were guided by science alone in their decision making.
As talk of a lockdown persisted, she looked out onto her vast warehouse filled with stacks of grocery store circulars, bags of chemical products and crates of detergent to ship to China. “The factory has to survive too,” she said.
Business leaders, and even the Alzano Lombardo mayor, resisted a lockdown, telling the local newspaper that it would be a tragedy for the economy and contacting their commercial associations with influence in Rome.
In the capital, Mr. Conte stressed that he would be guided by science alone. He declined interview requests for this article but has denied ever receiving requests from Confindustria as his government weighed what to do in Bergamo.
The powerful industrial group’s own representatives said they made their requests clear.
“There was a direct line between Confindustria and the government at that time,” said Licia Mattioli, who was then the group’s vice president.
The leadership argued directly to Mr. Conte that the rapid lockdown of the factories in Lodi unnecessarily cost jobs and that in Bergamo’s factories steps like social distancing would be sufficient.
“What they were saying was that to stop all the industry, also locally, is really very, very dangerous,” she recalled.
“I don’t know if they understood,” she said of Mr. Conte and his ministers. “But they listened at least.”
The factories stayed open until late March, and many never closed.
“I can assure you that never, never, never we made considerations on this,” said Mr. Speranza, the health minister. “We decided since the beginning that the first point is health — everything else comes after.”
On March 3, the government’s scientific committee proposed a red zone around Nembro and Alzano Lombardo. The Lombardy authorities considered it a done deal. So did Mr. Cancelli, the Nembro mayor, who was now infected and working in isolation.
“This place should have been closed in February, when it became clear that there were officially declared cases in the hospital, that surely were in contact with health workers, relatives, other patients,” Mr. Cancelli said. “On March 3 we thought, ‘Now they will close tonight.’”
But Mr. Conte, who needed to approve the decision, has said that he didn’t hear of the plan for two more days.
A stretcher in the courtyard of the Pesenti Fenaroli hospital, which found itself at the center of the province’s outbreak.
In the meantime, Mr. Speranza said, he pressed the scientific committee for a report on their rationale for closing the towns. “They said only ‘Close,’” Mr. Speranza said. “You can’t say, ‘I take away the freedom of people,’ for two words.”
Confused by the terms about coronavirus testing? Let us help:
Antibody: A protein produced by the immune system that can recognize and attach precisely to specific kinds of viruses, bacteria, or other invaders.
Antibody test/serology test: A test that detects antibodies specific to the coronavirus. Antibodies begin to appear in the blood about a week after the coronavirus has infected the body. Because antibodies take so long to develop, an antibody test can’t reliably diagnose an ongoing infection. But it can identify people who have been exposed to the coronavirus in the past.
Antigen test: This test detects bits of coronavirus proteins called antigens. Antigen tests are fast, taking as little as five minutes, but are less accurate than tests that detect genetic material from the virus.
Coronavirus: Any virus that belongs to the Orthocoronavirinae family of viruses. The coronavirus that causes Covid-19 is known as SARS-CoV-2.
Covid-19: The disease caused by the new coronavirus. The name is short for coronavirus disease 2019.
Isolation and quarantine: Isolation is the separation of people who know they are sick with a contagious disease from those who are not sick. Quarantine refers to restricting the movement of people who have been exposed to a virus.
Nasopharyngeal swab: A long, flexible stick, tipped with a soft swab, that is inserted deep into the nose to get samples from the space where the nasal cavity meets the throat. Samples for coronavirus tests can also be collected with swabs that do not go as deep into the nose — sometimes called nasal swabs — or oral or throat swabs.
Polymerase Chain Reaction (PCR): Scientists use PCR to make millions of copies of genetic material in a sample. Tests that use PCR enable researchers to detect the coronavirus even when it is scarce.
Viral load: The amount of virus in a person’s body. In people infected by the coronavirus, the viral load may peak before they start to show symptoms, if symptoms appear at all.
The interior ministry notified Bergamo’s military police to begin preparations for a lockdown, according to Col. Paolo Storoni, then the head of the Carabinieri in the area. Carmen Arzuffi, the owner of Hotel Continental, said the local police prefect called on March 4 to book 50 rooms for 100 incoming officers.
On March 5, the scientific committee again urged the government to lock down the towns. Mr. Speranza said he sent Mr. Conte the report that night. A member of Parliament from Bergamo privately pressed Mr. Conte’s office about what was taking so long, arguing that a human catastrophe was unfolding.
Mr. Conte’s office replied, according to correspondence seen by The Times, that there would be a ministerial-level meeting on Saturday, two days later, and that no decision would come before then.
By March 6, law enforcement had begun setting up at the hotel.
The police filled the hours by inspecting the routes they were supposed to close off and holding briefings in the basement, with commanders drawing maps of the towns and their streets on an easel.
“They knew it all by heart,” Ms. Arzuffi, the hotel owner, said.
As they ran drills, Mr. Conte met on March 6 with the scientific committee in Rome yet again. According to Mr. Speranza, the committee told Mr. Conte that closing Bergamo was no longer the issue. All of Lombardy, including Milan, needed to be locked down.
Two days later, on March 8, Mr. Conte did just that.
Mr. Conte has portrayed himself as urging the scientists to think bigger and bolder, saying he told them, “Shouldn’t we think of more radical measures?”
Later that day, the police officers at the Hotel Continental packed up and left.
“Nothing happened,” Mr. Cancelli said.
The Virus Preyed
As the authorities decided what to do, the virus seemed to spread everywhere and touch everyone. Infections ravaged homes and apartments. People started dying.
Mr. Orlandi, the burly truck driver who had once delighted the children in his family by thumb wrestling them with his gaping hands, died the day after his family learned he had contracted the virus. Some of his family became infected and died, too.
Giuseppa Nembrini, 82, and Giovanni Morotti, 85, a married couple in two separate rooms down the hall from Mr. Orlandi, both died.
Angiolina Cavalli, 84, a patient across the hall, died as well. Her husband, Gianfranco Zambonelli, 85, who had visited the hospital, died of the virus, too.
“They never told us anything,” Francesco Zambonelli, their son, who also contracted the virus, said of the hospital. “I think without knowing it, we became a vehicle for contagion to others.”
Francesco Zambonelli’s mother died at Pesenti Fenaroli Hospital. Both he and his father, who died of coronavirus, visited her and contracted the virus.
The empty stadium of the Atalanta soccer club in Bergamo. Just before the outbreak was detected, some 40,000 Atalanta fans traveled to Milan for a big European game.
Some of the sick included Bergamo soccer fans, 40,000 of whom had commuted to Milan on Feb. 19 to cheer for their local team, Atalanta, in a Champions League match against the Spanish team Valencia.
“We were stuck one next to the other,” recalled Matteo Doneda, 49, a rabid fan of Atalanta, who sang at the game, “You’ll know when we do damage! We are Bergamaschi, and we know no limits!”
On Feb. 26, Mr. Doneda said cookies began “tasting like sand” and his wife drove him to a hospital. He could barely walk and soon found himself breathing from within an oxygen helmet, surrounded by elderly people gasping for air. He said some of them had broken jaws under their masks, from fainting and falling in the ward.
Dr. Avogadri declined and lost consciousness, eventually drifting into a semi-comatose state in an intensive care ward, as she lost half of her hair. “I wanted to die,” she said.
When she was finally discharged, she discovered that the doctor who managed to find her a swab at Pesenti Fenaroli Hospital had died and that her older sister, who lived nearby, lay in an intensive care unit, a breathing tube down her throat.
No One to Blame
All the authorities involved now recognize Bergamo’s losses as a tragedy. But invariably they lay blame for it elsewhere.
The World Health Organization says that it limited its case definitions for practical reasons, primarily not to waste resources at the outset of an uncertain contagion. The rationale, said Dr. Margaret Harris, a spokeswoman for the organization, was “to limit the testing to a specific population at risk.” It is a position that past W.H.O. officials considered reasonable.
But Dr. Harris also argued that when the agency updated the guidelines at the end of January, it made clear “that the patient’s doctor is the one, ultimately, to decide who to test.”
Doctors in Bergamo considered that a convenient caveat.
The guidance was “the thing that generated the huge problem of the spread of the pandemic,” Dr. Avogadri said. “It was a big limitation.”
Dr. Monica Avogadri, who pushed her colleagues to break protocol and test one of her patients for coronavirus, was sickened badly by the virus herself.
In Bergamo last month. The Italian government has introduced a series of restrictive measures throughout the nation to contain the second wave of the virus.
The W.H.O. “made a mistake,” said Giuseppe Ruocco, Italy’s chief medical officer and a senior official in its health ministry, adding that if Italy hadn’t automatically followed the organization’s lead it “could have certainly avoided cases and the infection of medical staff.”
In June, Italy bestowed a knighthood in the Order of Merit of the Italian Republic on Dr. Malara, the physician who exposed the outbreak by disregarding the protocol.
Local officials and bereaved families in Nembro and Alzano Lombardo argue that closing the towns in February would have slowed the spread. A local prosecutor is investigating what happened and what didn’t happen and why.
But the government would prefer to focus on its closing of Lodi and then the region.
“It’s two small towns that everyone now knows,” Mr. Speranza, the health minister, said when asked how it was possible the prime minister didn’t know for three days about the shutdown proposal in Bergamo. “But it’s two small towns.”
And Mr. Conte has dismissed questions about the boldness of his decision making.
“There was no delay,” he has insisted.
A Province Gutted
Today Bergamo is a province gutted by loss.
Earlier this month, the Rev. Matteo Cella, who performed many abbreviated funeral rites for families he knew, greeted widows and widowers, sons and daughters, nieces and nephews on the Day of the Dead.
Wearing blue surgical masks, they leaned against the gravestones of their loved ones, or alongside the wood crosses of the unfinished graves of coronavirus victims.
Father Cella and other prelates read the names of the 231 people who had died in Nembro since the previous November. At least 188 had succumbed to Covid-19. They read the name of Mr. Orlandi, and of the other patients and doctors and visitors with whom he shared the third floor of the hospital during his final days.
As the mourners followed the priests in prayers, some wandered to the mausoleum wall at the back of the cemetery. Familiar names filled the wall.
“Franco Orlandi,” read one. “1-3-1936 – 25-2-2020.”
In Nembro, where the mortality increased 850 percent, clergy read out the names of the dead during a Mass on Nov. 1, All Saints’ Day.
A Covid-19 patient undergoing rehabilitation being helped to walk by a nurse at the Bolognini hospital.
“It’s still astonishing,” said Luigia Provese, 81, who drank coffee at the same bar as Mr. Orlandi and said that three of the four people she played cards with had died from the virus. “These are all people I know.”
As the virus has exploded again throughout Italy, Bergamo’s massive infection rate during the first wave, doctors say, has given it a measure of immunity. Its hospitals, once an exporter of infection and the sick, are taking patients in from the surrounding areas.
On Nov. 2, Bergamo’s fairgrounds debuted as a newly converted intensive therapy ward. Dozens of beds radiated wires. Ventilators stood on standby. A team of nurses in hazmat gear huddled for a briefing about reserve oxygen tanks.
Their coordinator, Lauretta Rota, 56, looked on in disbelief.
“It took some time to believe this was happening all over again,” she said. “There is an emotional and physical exhaustion that comes with that knowledge of what we have to face.”
Her cellphone rang.
“OK,” she said, excusing herself. “The first patient is on the way.”
Emma Bubola contributed reporting from Bergamo and Rome.
Jason Horowitz is the Rome bureau chief, covering Italy
www.rainews.it/dl/rainews/articoli/Inchiesta-Bergamo-Pm-Nessuno-scontro-con-Oms-verifiche-solo-sul-piano-pandemico
Pm Bergamo: "Nessuno scontro con Oms, verifiche solo sul piano pandemico"
"Accertare l'esistenza o meno di un piano pandemico e quando sarebbe stato redatto", ecco perché sono stati convocati come persone informate dei fatti alcuni ricercatori dell'Oms, che non si sono presentati a deporre in quanto l'Organizzazione Mondiale della sanità ha invocato l'immunità diplomatica
La Procura di Bergamo ha chiesto al Ministero degli Esteri di chiarire se i ricercatori dell’Oms, chiamati a testimoniare nell'ambito dell’inchiesta sulla gestione della pandemia nella provincia più colpita d'Italia, godano dell' "immunità diplomatica", come comunicato ai magistrati nei giorni scorsi. "Nessun braccio di ferro con Oms" L'indagine della Procura di Bergamo, che ipotizza il reato di epidemia colposa, riguarda la mancata istituzione della zona rossa in Val Seriana e la chiusura e poi quasi immediata riapertura dell'ospedale di Alzano Lombardo. I magistrati hanno sentito nei mesi scorsi come persone informate sui fatti, tra gli altri, il presidente del Consiglio Giuseppe Conte, il ministro Roberto Speranza, il presidente della Regione Lombardia, Attilio Fontana.
Pur convocati, alcuni ricercatori dell'Oms non si sono presentati a deporre in quanto l'Organizzazione Mondiale della sanità ha invocato per loro l'immunità diplomatica. Il procuratore di Bergamo, interpellato dall'Ansa sulla vicenda, ha chiarito che non c'è alcun braccio di ferro in corso, "né alcuna indagine sull'Oms o sulle strutture tecnico-scientifiche o politiche oppure su politici italiani", e che l'unico interesse è "accertare l'esistenza o meno di un piano pandemico e quando sarebbe stato redatto. Questo è importante per le valutazioni che la procura sta facendo nell'ambito dell'indagine sull'ospedale di Alzano e sulla gestione dell'epidemia nella Bergamasca" durante i mesi di febbraio e marzo scorsi. La questione dell'immunità Come anticipato in un promo della puntata di 'Report' in onda il 30 novembre, l'Oms ha spedito da Copenaghen, sede europea, una nota alla Procura e ai ministri degli Esteri e della Salute, Luigi Di Maio e Roberto Speranza, in cui afferma che i suoi ricercatori non sono tenuti a rispondere alle domande dei magistrati per via del loro speciale status. Nel contempo, l'organizzazione ha pure invitato i suoi ricercatori a non presentarsi davanti ai pubblici ministeri, cosa che però alcuni di loro non hanno fatto recandosi in Procura e rispondendo pure alle domande dei pm. La Procura ha deciso di non rispondere alle note ricevute dall'Oms ma di avviare "un'interlocuzione" col Ministero degli Esteri per capire se effettivamente esista questa presunta immunità che viene fatta risalire alla Convenzione del 1947 sui privilegi e le guarentigie di chi fa parte delle agenzie dell'Onu.
Un'immunità che l'Oms ha ritenuto di non far valere per il vicepresidente europeo, Ranieri Guerra, convocato e sentito il 5 novembre scorso come persona informata sui fatti, anche su un rapporto di un centinaio di pagine redatto dalla sezione Oms di Venezia in cui si criticava il governo italiano per la gestione della prima fase dell'emergenza. Questo dossier, che faceva riferimento anche al mancato aggiornamento del piano pandemico del 2006, era rimasto online per poche ore e poi era 'sparito'. I nodi da sciogliere Il Ministero degli Esteri dovrà sciogliere alcuni nodi: se effettivamente esista un'immunità come quella invocata dall'Oms che arriva a configurare un "divieto di testimoniare", se questa immunità possa riguardare anche dei ricercatori contrattisti, quindi non funzionari come Guerra, per il quale invece non è stata reclamata. Da capire anche se eventualmente ai ricercatori possa essere imposto un silenzio tout court oppure se essi possano opporre solo un segreto su attività circostanziate svolte nell'ambito dell'Oms, analoghe a quello previsto per categorie come i giornalisti o i pubblici ufficiali.
ECCO, abbiamo iniziato parlando di cosa sia considerato COVID.
Ma adesso torniamo alle malattie infettive in generale.
Strane notizie dall'ISS: ma appena 3 anni fa non berciavano tanto per vaccinare chiunque dalla rosolia e dal terribile morbillo?
www.epicentro.iss.it/morbillo/bollettino/RM_News_2020
Dal 1 gennaio al 31 ottobre 2020, in Italia, sono stati segnalati, da 12 Regioni, 101 casi di morbillo (incidenza 3,3 casi per m ilione), di cui 52 nel m ese di gennaio, 40 nel mese di febbraio e 9 nel mese di marzo. Non sono stati segnalati casi da aprile 2020. L’età mediana dei casi è 33 anni. Sono stati segnalati cinque casi in bambini con meno di un anno di età. Il 93% dei casi per cui è noto lo stato vaccinale era non vaccinato al momento del contagio. Il 26% dei casi ha sviluppato almeno una complicanza. Sono stati segnalati 12 casi tra operatori sanitari e due casi tra operatori scolastici. Dal 1 gennaio al 31 ottobre 2020 sono stati segnalati 12 casi di rosolia (di cui 9 nel mese di gennaio e 3 nel mese di febbraio), da sei Regioni. L’età mediana dei casi è 33 anni.
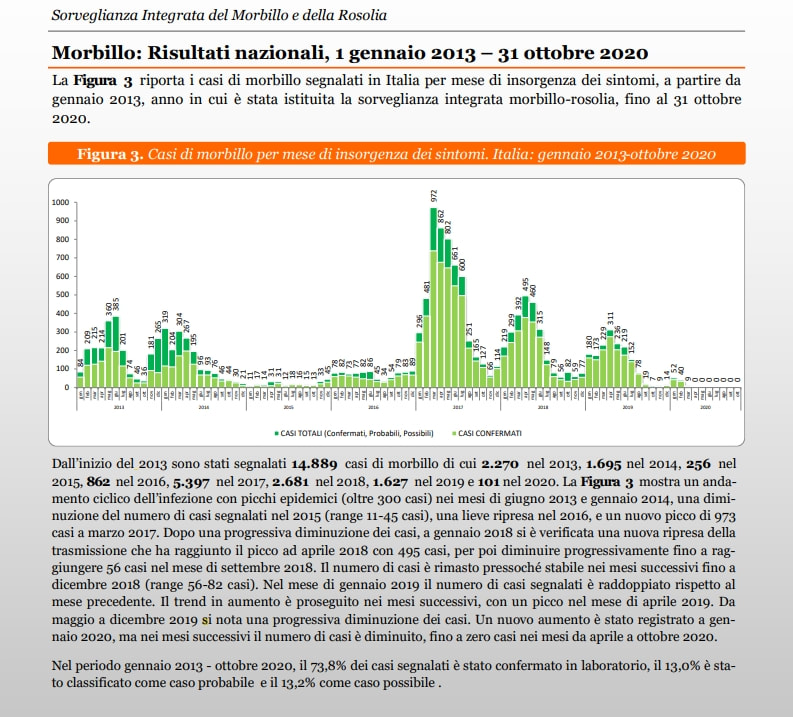
Dall’inizio del 2013 sono stati segnalati 14.889 casi di morbillo di cui 2.270 nel 2013, 1.695 nel 2014, 256 nel 2015, 862 nel 2016, 5.397 nel 2017, 2.681 nel 2018, 1.627 nel 2019 e 101 nel 2020. La Figura 3 mostra un andamento ciclico dell’infezione con picchi epidemici (oltre 300 casi) nei mesi di giugno 2013 e gennaio 2014, una diminuzione del numero di casi segnalati nel 2015 (range 11-45 casi), una lieve ripresa nel 2016, e un nuovo picco di 973 casi a marzo 2017. Dopo una progressiva diminuzione dei casi, a gennaio 2018 si è verificata una nuova ripresa della trasmissione che ha raggiunto il picco ad aprile 2018 con 495 casi, per poi diminuire progressivamente fino a raggiungere 56 casi nel mese di settembre 2018. Il numero di casi è rimasto pressoché stabile nei mesi successivi fino a dicembre 2018 (range 56-82 casi). Nel mese di gennaio 2019 il numero di casi segnalati è raddoppiato rispetto al mese precedente. Il trend in aumento è proseguito nei mesi successivi, con un picco nel mese di aprile 2019. Da maggio a dicembre 2019 si nota una progressiva diminuzione dei casi. Un nuovo aumento è stato registrato a gennaio 2020, ma nei mesi successivi il numero di casi è diminuito, fino a zero casi nei mesi da aprile a ottobre 2020. Nel periodo gennaio 2013 - ottobre 2020, il 73,8% dei casi segnalati è stato confermato in laboratorio, il 13,0% è stato classificato come caso probabile e il 13,2% come caso possibile .
QUINDI, tutto 'sto casino per il DL Lorenzin... e poi vedi che:
-2013, 2.270 casi;
-2014: 1.695
-2015: 256
-2016: 862
-2017: 5.397
-2018: 2.681
-2019: 1.627
-2020: 101
QUINDI QUINDI QUINDI, quando quella strega della Lorenzin parlava della terribile epidemia di Morbillo diceva cazzate, no? Alla fine, nel 2019 c'erano più casi che nel 2015 e del 2016 messi insieme! E meno male che era già entrato in vigore il DL Lorenzin. Chiarissimamente non DL non molto ispirato ad una 'vera emergenza' epidemiologica, visto che i picchi sono andati avanti e indietro per anni e picchi come quello del 2017 erano già presenti, se ricordo bene, nel 2008 e nel 2012 circa.
In altre parole, per come la vedo io, la situazione è stata questa:
-2014: l'Italia viene scelta come avanguardia per le campagne vaccinali
-2015: la Glaxo minaccia di andarsene via dall'Italia, però presto ritorna sui suoi passi stanziando 1 MLD per i suoi stabilimenti, di cui mezzo per quello di Siena. Che proprio allora era nel mezzo della bufera per il crack MPS. E pensate che il PD renziano, all'epoca in auge, non ci facesse caso, all'offreta Glaxo?
-2016: si cominciano a cercare ragioni per aumentare i così pochi vaccini obbligatori: prima si iniziano le campagne mediatiche con alcuni casi di meningite, che però... sono troppo pochi. Ma intanto hanno aperto una discussione nell'opinione pubblica.
-2017: la fortuna vuole che dal mazzo si peschi un'altra carta, il ben conosciuto morbillo. E iniziano campagne di stampa ma anche Web (VaccinarSì, Medbunker, debunker vari, siti istituzionali, partitici, FB...) per favorire un nuovo DL che sarà varato con il nome di una quasi omonima di quel Francesco De Lorenzo (per la cronaca ancora iscritto all'Ordine dei medici, quanto meno fino a qualche anno fa) che prese la famosa stecca per il vaccino dell'epatite B. Nel mentre cacciavano Gava e Miedico (maggio 2017). Non avevano reati penali, ma l'Ordine dei medici li cacciò via ugualmente per le loro posizioni sui vaccini. Ma nel contempo si tengono un'assassina che ha ammazzato la moglie del suo ex amante (anche lui dottore; lei ha fatto solo 6 anni di galera a far tanto e adesso lavora in un P.S, benché più che con i bisturi, abbia a che fare con i coltelli... nella sua pagina FB dice che la vita è tutta un equilibrio sopra la follia...). E si tengono De Lorenzo. E quando chiesi numi a MedBunker (al secolo SalvodisGrazia) mi rispose che non lo hanno radiato perché non era richiesto 'dalla sentenza'. Eh già, perché Miedico e Gava erano stati condannati, eh?!?
-2018: con i nuovi salvifici vaccini sembrava che fossimo tutti salvi. Addirittura c'era gente che diceva che il crollo dei casi d'estate, era dovuto agli effetti del DL Lorenzin: in altre parole, i casi, che già erano declinati da oltre 900 di marzo a meno di 600 di luglio, ad agosto scesero a circa 200 e meno ancora nei mesi successivi. E dicevano SERIAMENTE (?) che era l'effetto delle prime vaccinazioni. Di un DL approvato a fine luglio.
E invece, nel 2018 torniamo ai picchi che non si vedevano dal luglio precedente. Non è pazzesco?
Per la Rosolia non è tanto diverso.
E il bello è, che da quando c'é il COVID... puff, sparito il morbillo e più o meno anche la rosolia. Ma si può seriamente credere a dati del genere? E sopratutto, a che pro vaccinare obbligatoriamente per malattie che continuano ad esistere nel corso degli anni senza apparentemente alcuna vera flessione?
 |  |
